A COPD patient’s breathing rate creeps up, his oxygen saturation drops to 86%, and he’s leaning over the bedside table trying to catch his breath. Reach for the wrong oxygen setting here, or miss the early warning signs, and a manageable moment turns into a rapid response call. Solid COPD nursing interventions depend on knowing exactly what comes first, from initial assessment through long-term COPD patient care.
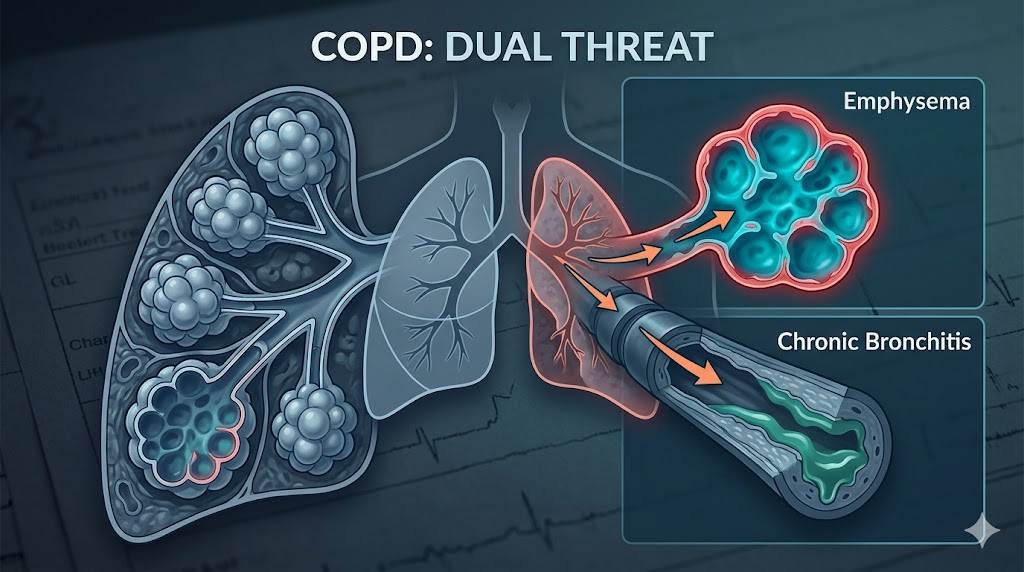
What Happens to the Lungs in COPD
COPD layers two problems on top of each other. Emphysema destroys the alveolar walls, so the lungs lose elastic recoil and trap air. Chronic bronchitis inflames the airway lining and packs it with thick mucus, narrowing an already struggling passage. Together, they block airflow in both directions, drive up CO2, and drop oxygen exchange — the root of nearly every symptom you’ll see at the bedside.
The scale is bigger than most nurses realize: the World Health Organization ranks COPD as the third leading cause of death worldwide, recording 3.4 million deaths in 2023. The 2025 GOLD guidelines confirm diagnosis with a post-bronchodilator FEV1/FVC ratio under 0.7, then grade severity by FEV1 percent predicted, from GOLD 1 (mild, ≥80%) to GOLD 4 (very severe, under 30%).
Priority Assessment in COPD Patient Care
Good COPD patient care starts before any intervention. Compare these findings against the patient’s own baseline, not a generic “normal”:
- Respiratory rate, depth, rhythm, and accessory muscle use
- SpO2 — many stable COPD patients run 88–92%, not 95–100%
- Lung sounds in every field: wheezes, crackles, or quiet spots
- Cyanosis, clubbing, barrel chest, or tripod positioning
- Mental status and capillary refill (confusion can mean CO2 buildup, not just fatigue)
- Recent ABG, sputum culture, or chest x-ray results
Building a Nursing Care Plan for a COPD Patient
A solid nursing care plan for COPD patient management centers on a handful of recurring diagnoses — match the intervention to whichever one is driving the current presentation:
- Ineffective Airway Clearance — excess mucus and a weak cough
- Impaired Gas Exchange — alveolar-capillary changes from emphysema
- Ineffective Breathing Pattern — airway obstruction and ventilatory muscle fatigue
- Activity Intolerance — mismatch between oxygen supply and demand
- Anxiety — dyspnea and a real fear of not being able to breathe
- Imbalanced Nutrition: Less Than Body Requirements — extra energy spent just breathing
COPD Nursing Interventions That Matter Most
These are the COPD nursing interventions that do the heaviest lifting once you’ve assessed the patient and matched the diagnosis.
1. Clear the airway. Teach pursed-lip breathing first: in through the nose for two counts, out through pursed lips for four. Add controlled “huff” coughing — a deep breath, a brief hold, then short forceful bursts — to clear mucus without exhausting the patient. Reinforce incentive spirometer use, ten breaths every waking hour, and watch for patients who blow into it instead of inhaling.
2. Get the oxygen target right. Aim for SpO2 88–92%, not 95–100%. Pushing saturation higher can worsen CO2 retention through ventilation-perfusion mismatch and the Haldane effect. Use a Venturi mask for precise FiO2 during a flare, titrate up only as needed, and wean gradually rather than shutting oxygen off the moment a number looks good.
3. Position for easier breathing. Default to high Fowler’s for routine care. When dyspnea spikes, guide the patient into tripod position — leaning forward with forearms supported — to stabilize accessory muscles and make each breath count.
4. Administer and teach medications. Bronchodilators (albuterol, salmeterol) and anticholinergics (ipratropium) relax airway smooth muscle, but only work if inhaler technique is correct — check it every time. After inhaled corticosteroids like beclomethasone, instruct patients to rinse and spit to prevent oral candidiasis. Pair mucolytics like acetylcysteine with fluids and huff coughing.
5. Support nutrition without adding to the workload. Offer five or six small, high-calorie, high-protein meals instead of three large ones — a full stomach pushes against the diaphragm and adds to the work of breathing. Limit beans, carbonated drinks, and cruciferous vegetables if bloating is a concern.
6. Break the anxiety-dyspnea cycle. Dyspnea triggers anxiety, which speeds breathing and deepens the dyspnea. Stay in the room, coach pursed-lip breathing in a calm voice, screen for anxiety and depression at routine visits, and refer to pulmonary rehabilitation for lasting improvement.
7. Catch an exacerbation early. Watch for rising sputum volume, a color change toward yellow or green, increased dyspnea, and a more frequent cough. Once a flare is underway, expect nebulized bronchodilators, systemic corticosteroids, and antibiotics as ordered — and watch closely for confusion or paradoxical breathing, which signal impending respiratory failure.
8. Plan for long-term COPD management nursing. A written action plan with green/yellow/red zones gives patients a clear script for home: what’s normal, what needs extra medication, and what means calling the provider or going to the ER. Revisit smoking cessation at every visit, confirm flu/pneumococcal/COVID vaccination status, and review home oxygen fire safety for anyone using tanks.
Evaluating Success in COPD Patient Care

Track specific markers instead of a general sense that things look better: SpO2 within the patient’s target range, correct inhaler technique without prompting, a written action plan the patient can explain back, and daily activities completed without dyspnea stopping them. Revisit these at every visit — COPD only moves in one direction, so today’s numbers become next month’s benchmark.
Fast CE For Less maintains a growing library of respiratory-focused nursing CE courses with no test required for a certificate. Check the current catalog at fastceforless.com for titles and contact hours that fit your renewal.
Pick one habit from this guide to start today: before touching a COPD patient’s oxygen flow rate, confirm their target SpO2 range first. That single check prevents more harm than nearly anything else on this list.
FAQs
What’s the priority nursing intervention for COPD?
Assess airway and breathing first, then position the patient upright or in tripod position before titrating oxygen toward their target range.
What SpO2 is normal for a COPD patient?
Most stable patients run 88–92%, lower than the 95–100% expected without lung disease. Pushing saturation higher can worsen CO2 retention.
What nursing diagnoses matter most in COPD patient care?
Ineffective Airway Clearance, Impaired Gas Exchange, Ineffective Breathing Pattern, and Activity Intolerance, with Anxiety and Imbalanced Nutrition joining as disease progresses.
Why is high-flow oxygen risky for COPD patients?
Excess oxygen worsens CO2 retention through ventilation-perfusion mismatch and the Haldane effect, not by simply suppressing the drive to breathe. Titrate to target instead of running a fixed flow rate.
What should discharge teaching cover?
Inhaler technique, pursed-lip breathing, a written action plan, smoking cessation resources, vaccination status, and home oxygen safety.

