Burn emergencies are unforgiving — every minute without proper intervention deepens tissue damage, accelerates shock, and narrows the survival window. Yet many nurses enter these situations without a clear burn emergency management framework, leaving critical steps like fluid resuscitation in burn patients and thermal injury assessment nursing to guesswork under pressure.

That gap costs lives. Without structured burn shock management, patients spiral into irreversible organ failure before surgical teams even arrive.
This guide gives acute care nurses a precise, evidence-based roadmap — from initial assessment through ICU stabilization — so the right actions happen in the right order, every time.
Understanding the Severity: Thermal Injury Assessment in Nursing
Before any treatment begins, accurate assessment is the foundation of burn injury management nursing care. The first step is determining the depth and extent of the burn.
Clinicians classify burns by depth:
- Superficial (first-degree): Affect only the epidermis; red, dry, and painful (e.g., sunburn)
- Partial thickness burns: Involve the epidermis and part of the dermis; blistered, moist, and intensely painful
- Full thickness burns: Destroy all layers of the skin; may appear waxy, leathery, or charred — often painless due to nerve damage
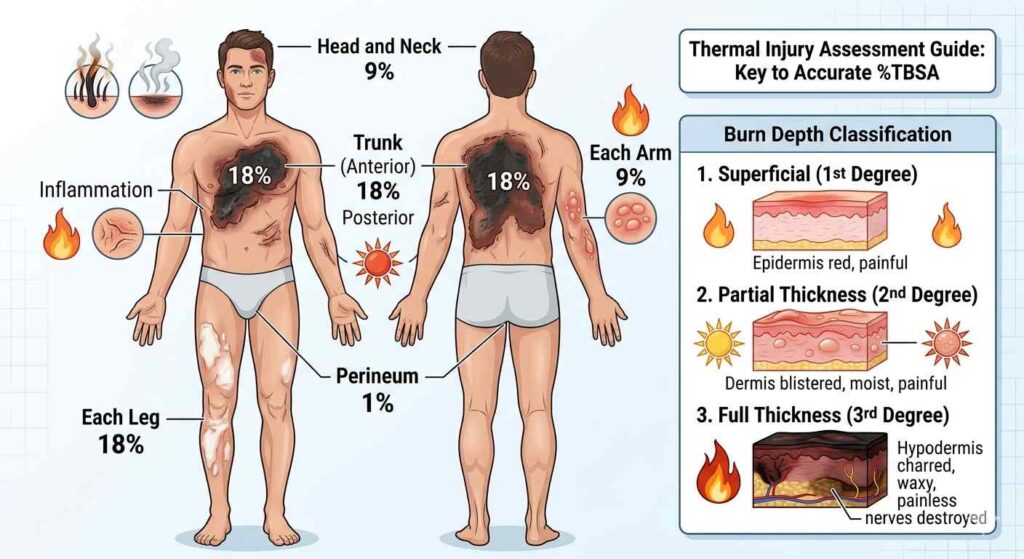
The Rule of Nines is a standard tool nurses use to estimate total body surface area (TBSA) burned. The Rule of Nines divides the adult body into regions each representing 9% or multiples thereof — head (9%), each arm (9%), each leg (18%), anterior trunk (18%), posterior trunk (18%), and perineum (1%). Accurate TBSA calculation directly informs fluid replacement decisions.
The First 24 Hours: Why Timing Is Everything in Burn Shock Management
The body’s response to a major burn is rapid and aggressive. Massive hypovolemic shock in burns begins almost immediately as fluid shifts from the intravascular space into the interstitium. This phenomenon, driven by inflammatory mediators and increased capillary permeability, is what makes burn shock management a top clinical priority.
Nurses must recognize the signs: tachycardia, hypotension, decreased urine output, altered mental status, and cool extremities. These are signals that fluid replacement therapy nursing interventions must begin without delay.

The critical window — the first 24 hours burn care guidelines — sets the pace for resuscitation. Inadequate fluid causes organ hypoperfusion and increased mortality; excessive fluid can lead to pulmonary edema, abdominal compartment syndrome, and worsening outcomes.
Parkland Formula: The Nurse’s Calculation Guide
The cornerstone of fluid resuscitation in burn patients is the Parkland formula. Understanding and applying the Parkland formula nursing calculation correctly is an essential competency for any nurse managing burn patients.

Formula:
4 mL × Weight (kg) × %TBSA burned = Total fluid (Lactated Ringer’s) in first 24 hours
Nurses administer the calculated volume in a specific pattern:
- First 8 hours: Half the total volume (calculated from time of injury, not time of arrival)
- Next 16 hours: Remaining half
For example, a 70 kg patient with 40% TBSA burns requires: 4 × 70 × 40 = 11,200 mL of Lactated Ringer’s over 24 hours — approximately 700 mL/hr in the first 8 hours.
This is why burn patient monitoring in emergency settings is so demanding. Nurses must continuously track intake/output, reassess hemodynamic status, and adjust infusion rates accordingly.
Airway Management: The Priority Above All Else
In any emergency burn treatment protocol, securing the airway takes precedence. Airway management in burn patients is critical because inhalation injuries cause airway edema that can progress rapidly, leading to complete obstruction within hours.
Red flags for inhalation injury include:
- Singed nasal hairs or eyebrows
- Carbonaceous sputum
- Stridor or hoarseness
- Burns to the face, mouth, or oropharynx
- History of burn in an enclosed space
Nurses should anticipate early intubation orders for patients showing any of these signs. Delaying intervention can make intubation impossible as edema worsens. High-flow humidified oxygen, continuous pulse oximetry, and capnography are all standard components of the emergency burn treatment protocol.
ICU Care and Wound Management for Severe Burns
Patients with burns exceeding 20% TBSA, full-thickness burns, inhalation injuries, or burns involving critical areas (hands, face, feet, genitalia) typically require ICU care for severe burns. In the ICU, nurses manage multi-system complications including infection, respiratory failure, coagulopathy, and nutritional deficits.
Burn wound care and dressing changes are among the most frequent and clinically important nursing tasks. Clean technique, appropriate dressing selection, and timely changes help prevent infection — a primary driver of mortality in burn survivors.
Eschar formation and debridement care is another critical consideration. Eschar — the dry, leathery tissue that forms over deep burns — can create circumferential constriction that impairs circulation or breathing. Nurses must assess for signs of compartment syndrome and prepare patients for escharotomy when needed. Surgical debridement, often followed by skin grafting, begins the path toward wound closure.
Burn patient monitoring in emergency settings continues in the ICU with close tracking of:
- Hourly urine output (goal: 0.5–1 mL/kg/hr in adults)
- Core temperature (burn patients are highly susceptible to hypothermia)
- Serum electrolytes, especially sodium and potassium
- Wound appearance and signs of infection (increased erythema, purulent discharge, fever)
Continuing Education and Clinical Competency
Managing burn emergencies is a high-stakes skill that requires ongoing learning. Nurses seeking to strengthen their knowledge in burn injury management nursing care and related acute care topics can benefit from accessible, accredited continuing education platforms. Completing CE courses on topics like fluid replacement therapy nursing, thermal injury assessment nursing, and burn shock management ensures that clinical knowledge stays current and evidence-based.
Continuing education in burn care helps nurses deliver safer, more effective care. Look for accredited CE courses by Fast CE For Less, in that course we cover emergency burn treatment protocols, fluid resuscitation, and acute care nursing competencies to advance your practice.
FAQs
Should the Parkland formula calculation start from the time of injury or hospital arrival?
Always from the time of injury. If a patient arrives 2 hours post-burn, the first-8-hour bolus window is already partially elapsed — nurses must back-calculate and increase the infusion rate to deliver the remaining volume within the correct timeframe. Missing this distinction is one of the most common errors in fluid resuscitation in burn patients.
Can burn patients feel pain in full thickness areas, and how does that affect pain management?
No — full thickness burns destroy nerve endings, making those zones painless. However, surrounding partial thickness burns remain acutely sensitive. Nurses must account for this “pain map” when planning analgesia; undertreating peripheral partial-thickness areas is a frequent gap in burn wound care and dressing changes.
What is the urine output target during fluid resuscitation, and what does deviation indicate?
Target is 0.5–1 mL/kg/hr in adults. Output below this signals under-resuscitation and worsening hypovolemic shock in burns; output above 1 mL/kg/hr suggests over-resuscitation, which raises the risk of pulmonary edema and abdominal compartment syndrome. Urine output is the primary real-time gauge nurses use to titrate IV rates.
How does circumferential eschar differ from non-circumferential, and what is the nurse’s role?
Circumferential eschar formation on limbs or the chest can restrict circulation or breathing — a surgical emergency requiring escharotomy. Nurses must assess distal pulses, capillary refill, and chest excursion every 1–2 hours. Documenting a new pulse deficit or declining SpO₂ in a chest-burn patient warrants immediate escalation — delaying escharotomy causes irreversible ischemia.
Are there burn populations where the standard Parkland formula is adjusted?
Yes. Children require a modified formula (Galveston formula) that accounts for higher surface-area-to-weight ratios and adds maintenance fluids. Elderly patients and those with cardiac or renal history need more conservative resuscitation to avoid fluid overload. Inhalation injury also increases overall fluid requirements beyond the standard Parkland calculation. These nuances are critical in ICU care for severe burns and often require multidisciplinary titration beyond the standard calculation.

