Contact Hours: 2
This educational activity is credited for 2 contact hours at completion of the activity.
Course Purpose
To provide mandated reporters of child abuse with an overview of the following:
- When legally required to call the SCR
- When children and families may be more appropriately assisted through community-based services or other supports
- Reduce bias in the decision-making process of whether a call must be made to the SCR
- The impact of trauma and Adverse Childhood Experiences (ACEs) on children and families
- Protective factors and the supports that can be referred to families to in lieu of making a report.
Overview
Child abuse and neglect are serious public health concerns. It involves the emotional, sexual, physical abuse, or neglect of a child under the age of 18 by a parent, custodian, or caregiver that results in potential harm, actual harm, or a threat of harm. This independent study provides an overview of child abuse, adverse childhood experiences, implicit bias, and the New York regulations for a mandated reporter to report child abuse and neglect.
Course Objectives
By the end of this learning activity, the learner will be able to:
- Be able to determine if a child shows indicators of maltreatment or abuse, including in a virtual setting.
- Recognize the signs of intellectual and/or developmental disabilities in children and factors to consider when determining whether a child with intellectual and/or developmental disabilities shows indicators of maltreatment or abuse.
- Recognize the impact of trauma and ACEs on children, families, and the mandated reporter.
- Recognize the mitigating effects of the five protective factors on trauma.
- Recognize the impact of bias on decision-making.
- Understand when a mandated reporter has a legal obligation to call the SCR.
- Recognize how the mandated reporter may better connect individuals and families with services.
- Know how to prepare to make the call to the SCR.
- Know how to complete the LDSS 2221A form.
- Understand rights as a mandated reporter.
Policy Statement
This activity has been planned and implemented in accordance with the policies of FastCEforless.com.
Disclosures
Fast CE For Less and its authors have no disclosures. There is no commercial support.
To access 2025 NYSED Identification and Reporting of Child Abuse and Maltreatment/Neglect, purchase this course or a Full Access Pass.
If you already have an account, please sign in here.
To access 2025 NYSED Identification and Reporting of Child Abuse and Maltreatment/Neglect, purchase this course or a Full Access Pass.
If you already have an account, please sign in here.
| Adverse Childhood Experiences (ACE) | Traumas that happen before age 18, such as abuse, neglect, or family problems. |
| Child Abuse | Involves the emotional, sexual, physical, or neglect of a child under the age of 18 by a parent, custodian, or caregiver that results in potential harm, harm, or a threat of harm. |
| Domestic Violence | The victimization of an individual with whom the abuser has an intimate or romantic relationship. It includes physical violence, sexual violence, stalking, and psychological aggression (including coercive acts) by a current or former intimate partner. |
| Emotional Abuse | Refers to behaviors that harm a child’s self-worth or emotional well-being. Examples include name calling, shaming, rejection, withholding love, and threatening. |
| Implicit Bias | A negative attitude, of which one is not consciously aware, against a specific social group. |
| Intellectual and/or Developmental Disabilities | Differences that are usually present at birth and that uniquely affect the trajectory of the individual’s physical, intellectual, and/or emotional development. |
| Joint Commission on Accreditation of Healthcare Organizations | Enables and empowers health care organizations around the world to build a foundation for quality care and patient safety. |
| Local Child Protective Services (CPS) | A branch of your state’s social services department that is responsible for the assessment, investigation and intervention regarding cases of child abuse and neglect, including sexual abuse. |
| Mandated Reporter | An individual who holds a professional position that requires them to report to the appropriate state agency cases of child abuse that they have reasonable cause to suspect. |
| Munchausen By Proxy Syndrome | Factitious disorder where an individual fabricates or exaggerates mental or physical health problems in the person for whom he or she cares. The primary motive is to gain attention or sympathy for themselves. |
| Neglect | The failure to meet a child’s basic physical and emotional needs. These needs include housing, food, clothing, education, and access to medical care. |
| Office Of Children And Family Services (OCFS) | Serves New York’s public by promoting the safety, permanency and well-being of children, families and communities, and achieves results by setting and enforcing policies, building partnerships, and funding and providing quality services. |
| Physical Abuse | The intentional use of physical force that can result in physical injury. Examples include hitting, kicking, shaking, burning, or other shows of force against a child. |
| Sexual Abuse | Involves pressuring or forcing a child to engage in sexual acts. It includes behaviors such as fondling, forced anal, oral, or vaginal penetration and exposing a child to other sexual activities. |
| Statewide Central Register Of Child Abuse And Maltreatment (SCR Or Central Register) | Also known as the “hotline” for reports made pursuant to the Social Services Law. The SCR receives telephone calls alleging child abuse or maltreatment within New York State. |
| Sentinel Injury | Visible, minor, and poorly explained injuries in young infants that raise concern for abuse. |
Family and Domestic violence are a common problem in the United States and affects approximately 10 million people every year. They are abusive behaviors in which one individual gains power over another individual. Domestic and family violence occurs among all ages, races, and sexes. It knows no cultural, educational, geographic, religious, or socioeconomic limitation. Domestic and family violence includes child abuse, intimate partner abuse, and elder abuse and encompasses economic, physical, sexual, emotional, and psychological abuse toward children, adults, and elders. ⁴˒⁵ It causes diminished psychological and physical health and decreases the quality of life.
Child abuse and neglect are serious public health concerns. Child abuse includes all four types of abuse and neglect against a child under the age of 18 by a parent, caregiver, or another person in a custodial role that results in harm, potential for harm, or threat of harm to a child. The four common types of abuse and neglect include emotional abuse, physical abuse, sexual abuse, and neglect.
In the 1980s, a national study was conducted and concluded that many professionals did not report abuse and maltreatment because of a lack of knowledge in recognizing warning signs and clues of abuse, and confusion regarding the reporting laws and procedures. In 1999, the Monroe County Department of Social Services engaged the University of Rochester’s Department of Community and Preventive Medicine and the Perinatal Network of Rochester to conduct research for a campaign to increase community involvement to prevent child abuse and maltreatment, and to improve reporting. Mandated reporters were included as a group in this study. As a result of these and other studies, there is evidence that child abuse and maltreatment are underreported and that, conversely, some situations that are reported to the New York State Central Register (SCR) are more suitable for preventive services or other resources. The purpose of this training is to provide the mandated reporter with the knowledge to make an informed decision about whether a situation involves child abuse or maltreatment, what the reporting obligation is, and how to go about making such a report. This training is designed to provide an understanding of the preventive-protective continuum of care within the Child Protective Services (CPS) system as it operates in New York State.
Shared Mission
The State’s Office of Children and Family Services (OCFS), the Statewide Central Register of Child Abuse and Maltreatment (SCR or Central Register), local child protective services (CPS) agencies and mandated reporters promote the well-being of New York’s children, families and communities. 12
Article 6, Title 6 of the Social Services Law, which is titled “Child Protective Services,” establishes the New York Statewide Central Register of Child Abuse and Maltreatment (SCR or Central Register), informally referred to as “the child abuse hotline” or “the hotline.” 12 The Central Register, administered by New York State’s Office of Children and Family Services, is how mandated reporters make reports of suspected child abuse and neglect. A mandated reporter is an individual whose profession is listed in the social services law and who is legally required to report to the Central Register whenever they believe or suspect that a child has been abused or neglected. A concerned citizen of the public can also make suspected child abuse or neglect reports.
Title 6 also sets up the structure of the child protective system at the local level. 12 Each county must provide a local child protective service agency to investigate reports accepted by the Central Register regarding children living within that county. New York City is considered a single district, and its child protective services are provided by the Administration for Children’s Services (ACS).
Families in crisis may not meet the legal criteria required to call the SCR and may be better served by being connected to a variety of community services in their area. The Family Assessment Response (FAR) is New York State’s alternative child protective response to some reports of child abuse or neglect. The family assessment response does not require an investigation and determination of allegations, or culpability for families reported to the SCR. 12 It is an alternative approach to providing protection to children by engaging families in an assessment of child safety and family needs, finding solutions to family problems, identifying support to meet the family’s needs, and increasing their ability to care for their children. Other resources include: 12
For more information on what services are available for children and parents in your community, visit https://nysmandatedreporter.org
The OCFS H.E.A.R.S. – Help, Empower, Advocate, Reassure and Support – Family line assists families by providing resources and referrals to a variety of services such as food, clothing, housing, childcare, parenting education and more. Representatives are available to help Monday through Friday 8:30am-4:30pm at 888-554-3277.
OCFS lists on its website resources on adverse childhood experiences, including information on how to access a wide variety of services at https://ocfs.ny.gov/programs/cwcs/aces.php
NY Project Hope provides emotional support for New York State residents. This includes an Emotional Support Helpline (1-844-863-9314), Online Wellness Groups, and a website filled with supportive resources (NYProjectHope.org).
The New York State Office for the Prevention of Domestic Violence has a website that provides a number of resources for people who may be experiencing, or are survivors of, domestic violence: https://opdv.ny.gov/survivors-victims
Prevent Child Abuse New York also has a prevention and parent helpline available for parents and caregivers that is confidential and multi-lingual and can refer or connect caregivers to community-based services. This helpline is available Monday through Friday from 9am-4pm at 1-800-CHILDREN.
Parents and caregivers may also call 2-1-1, operated by the United Way, for health and human services information, referrals, assessments, and crisis support to help them find the assistance they need to address the everyday challenges of living, as well as those that develop during times of disaster or other community emergencies. 2-1-1 is multi-lingual and available 24 hours a day 7 days a week.
Trauma
Trauma is an intense event that threatens a person’s life or safety in a way that is too much for the mind to manage and leaves the person powerless. For instance, for many parents, having a child removed from the home and dealing with the child welfare system are traumatic events. Trauma can bring about physical reactions such as rapid heart rate, tense muscles, or shallow breathing. Common traumatic events include: 12,13,24
- Emotional abuse
- Family violence
- Sexual abuse
- Violence in the community
For many parents, having a child removed from the home and dealing with the child welfare system are traumatic events.
Adverse Childhood Experiences (ACE)
Adverse Childhood Experiences (ACE) are negative experiences that occur during childhood that can increase the likelihood of risk-taking behavior later in life. 5,18 A better understanding of how a high ACE score can increase risk-taking behavior has been explored through research. The CDC-Kaiser Permanente Adverse Childhood Experiences Study is one of the largest investigations of childhood abuse and neglect and household challenges, and later-life health and well-being. The original ACE Study was conducted at Kaiser Permanente from 1995 to 1997. Over 17,000 health members from Southern California who received physical exams completed confidential surveys regarding their childhood experiences and current health status and behaviors. The ACE questionnaire asked difficult questions regarding the first 18 years of life. Questions were related to physical, emotional, and sexual abuse, and the frequency of such occurrences. The suicide of a family member, drug addiction, and mental health issues played roles in the calculation of the score. ACE scores ranged from zero to 10, with zero representing no exposure. 5,18
The study uncovered how adverse childhood experiences are strongly related to the development of risk factors for disease and well-being throughout life. 5,18 It also found that ACEs are common across all populations, however some populations are more vulnerable to experiencing ACEs because of the social and economic conditions in which they live, such as poverty, experiencing racism, having generational trauma, and experiencing frequent unintended or indirect discrimination. Almost 66% of study participants reported at least one adverse childhood experience and more than 20% reported three or more adverse childhood experiences. The study found that children who experience numerous adverse experiences are more likely to have higher rates of negative health outcomes later in life, including depression, obesity, substance use, anxiety, heart disease and early death. In addition, toxic stress can impact a child’s behavior and development. 5,18 Toxic stress occurs when a child experiences severe, prolonged adversity without adequate support, having a significant negative impact on adverse childhood scoring. Toxic stress means that the stress response stays continuously activated in the body, which negatively impacts a child’s development and behavior. The ACE Pyramid conceptualizes the framework for the ACE study as it relates to individual health and well-being across the lifespan, from conception to death.

According to the adverse childhood experiences Pyramid, neurodevelopment is disrupted or stunted following an adverse childhood experience. Social, emotional, and cognitive impairments result, which progress to high-risk behaviors that negatively impact overall health. Disease, disability, and social problems ensue, cascading to an early death. Therefore, there is a correlation between a higher ACE score and an increased risk of poor physical and mental health due to poor choices, risky behaviors, and social issues. 5,18 For more information on ACEs, visit https://ocfs.ny.gov/programs/cwcs/aces.php
Trauma-Informed Practice
Mandated reporters must know many people have a history of trauma. Trauma-informed practice is a model for engaging with children and families, while also recognizing the influence and impact that past or present trauma may have. In trauma-informed practice, a mandated reporter should not question or “bring up” past traumatic experiences, but rather assume that traumatic experiences may have occurred, and tailor questions accordingly. For example, a healthcare professional should ask for permission before touching a patient, explain why a physical exam must be performed, and explain why sensitive questions must be asked.24 The goals of a trauma-informed practice are to avoid the inadvertent retraumatization of individuals, and for the mandated reporter to understand that trauma may have an impact on a person’s behavior, and their own.
Trauma can significantly impact the work of mandated reporters, and it should be assumed that trauma may also have an impact on the child or family that the mandated reporter encounters. Adverse childhood experiences and trauma may not rise to the level of child abuse or maltreatment, however its impact on a child should be assessed, and the effects of adverse childhood experiences should be reduced through protective factors and resources, such as:12,24
Prevent Child Abuse NY www.preventchildabuseny.org
Center for the Study of Social Policy www.cssp.org
National Center for PTSD: www.ptsd.va.gov
National Child Traumatic Stress Network: www.nctsn.org
New York State Trauma-informed Network: https://www.traumainformedny.org/Home
OCFS Adverse Childhood Experiences (ACEs): https://ocfs.ny.gov/programs/cwcs/aces.php
Parents Anonymous: www.parentsanonymous.org
Implicit bias refers to attitudes or stereotypes that affect our understanding, actions, and decisions in an unconscious way, making them difficult to control.15,18 It may present as biases against groups of people who have a different gender, sexual orientation, racial group, or ethnicity, and can occur anywhere, including the criminal justice system, healthcare system, schools, and workplace settings.
An implicit bias may be opposite of a person’s conscious beliefs without them realizing it, whereas explicit bias is a bias that an individual is aware of on a conscious level, for example, feeling threatened by a minority group, and bullying a member of the minority group as a result. It is important to understand that implicit bias can also become explicit bias. This occurs when an individual becomes consciously aware of the prejudices and beliefs that they possess, and then makes a conscious choice whether to act on those beliefs. 15,18
One of the main reasons people develop biases is because of the natural tendency of our brains to look for patterns and associations to make sense of the environment. Even as early as the age of five, children group people based on traits (race, skin color, sex), and can distinguish the differences among groups. The way people are raised can also contribute to implicit bias. Parental attitudes can influence a child’s thoughts and implicit prejudices. Likewise, siblings, school settings, and the cultural environment can all play a role in shaping beliefs and developing implicit biases. 15,18
National research has shown, and OCFS data has confirmed, that disparities exist throughout the child welfare system presently and historically. The OCFS’ Disproportional Minority representation (DMR) data has shown historical overrepresentation of children and families of color in the child welfare system. Families of color have also been more likely to be involved in a report to the SCR. Likewise, children of color have been more likely to be placed in foster care and generally have slower performance goals and achievements.
Research has also shown that the income status of families is a significant predictor of involvement with the child welfare system. For instance, families living below the poverty line are three times more likely to be substantiated for child maltreatment. This disparity has long-lasting and devastating impacts on both families and communities.
Families that have been investigated by CPS commonly have several poverty related risk factors such as:
- Food insecurity
- Housing instability
- Lack of access to childcare
- Single parenthood
- Unemployment
Unconscious prejudices and negative attitudes toward certain groups of people can compromise the mandated reporter’s decision-making, however, these biases can be unlearned. 15,18 The first step a mandated reporter can take to unravel their implicit bias is to understand their own world views. Bias can show up in a variety of ways. Bias might look like subconscious thoughts (implicit), conscious thoughts (explicit), stereotypes, or inaccurate judgements. Bias can, however, be unlearned. A proven strategy to reduce bias is to examine whether the facts of the situation would lead the mandated reporter to the same conclusion and decide to call the SCR if the demographic information for the child or family were different. For instance, the mandated reporter should consider if they would make the same decision to call if any of the following were different: 12, 15,18
- Age
- Culture
- Disability
- Ethnicity
- Gender
- Gender Identity or expression
- Immigration status
- Neighborhood where they reside
- Occupation
- Presence of a disability
- Primary Spoken Language
- Race
- Religion
- Sex assigned at birth
- Sexual Orientation
- Socio-economic status of the family
If the answer is yes, bias may be impacting the decision to call the SCR.
The best tool available to reduce bias is critical thinking. A mandated reporter must use critical thinking when deciding whether to call in a report to the SCR. Before making the report, the mandated reporter should:
- Identify specific concerns about the current situation.
- Gather adequate information about the current situation.
- Analyze that information to separate facts from assumptions.
- Recognize the possibility of bias in personal opinions.
- Develop multiple hypotheses that could explain the situation.
- Determine whether they are legally required to call the SCR and, if not, whether an alternative option is better, such as connecting the child or family to appropriate services in their community.
The mandated reporter should approach the situation with humility and recognize that although they may not know everything about the situation and the family, they must be open and willing to learn, approach their responsibility with empathy, compassion, care and curiosity, and consider information that may be different from first impressions and assumptions.
Harvard University developed the Implicit Association Test (IAT) which measures attitudes and beliefs, and can be accessed at https://implicit.harvard.edu/implicit/takeatest.html.
Causes of Child Abuse
Domestic and family violence, including child abuse often starts when a caretaker or parent feels the need to dominate or control a child. This can occur because of several reasons, such as: 13,14,16,17
- Alcohol and drugs use, as an impaired individual may be less likely to control violent impulses.
- Anger management issues.
- Learned behavior from growing up in a family where domestic violence was accepted.
- Personality disorder or psychological disorder.
While the research is not definitive, several characteristics are thought to be present in perpetrators of child abuse. Abusers tend to: 13,7,8,10
- Be nonbiological, transient caregivers in the home, such as a parent’s significant other.
- Have a history of substance abuse and/or mental health issues including depression in the family.
- Have a parental history of child abuse and or neglect.
- Have thoughts and emotions that tend to support or justify maltreatment behaviors.
- Lack understanding of children’s needs, child development and parenting skills.
- They have parental characteristics such as young age, low education, single parenthood, large number of dependent children, and low income.
There are several risk factors for child abuse, which are inclusive of individual, family, and community issues. For instance, there is a correlation between parental stress and child abuse. The more stress a parent experiences, such as separation or divorce, the more likely they will be involved in child abuse.
Exposure to domestic abuse and family violence as a child is commonly associated with becoming a perpetrator of domestic violence as an adult. 1,3,4 This cycle occurs because children who are victims or witness domestic and family violence may believe that violence is a reasonable way to resolve a conflict. As a child grows to become an adult, they may solve conflicts in a manner that is familiar to them, often resulting in a repeated cycle of domestic violence. Males who learn that females are not equally respected are more likely to abuse females in adulthood. Females who witness domestic violence as children are more likely to be victimized by their spouses. While females are often the victim of domestic violence, the gender roles can be reversed. Perpetrators of domestic violence commonly repeat acts of violence with new partners, and drug and alcohol abuse greatly increase these risks. Common risk factors for domestic violence include:1,3,4
- A family history of violence
- Aggressive behavior as a youth
- Antisocial personality disorder
- Corporal punishment in the household
- Domination, which may include emotional, physical, or sexual abuse that may be caused by an interaction of situational and individual factors. This means the abuser learns violent behavior from their family, community, or culture. They see violence and are victims of violence.
- Economic stress in families with low annual incomes
- Females whose educational or occupational level is higher than their spouse’s
- History of abuse as children
- Individuals with disabilities
- Low education
- Low self-esteem
- Marital discord
- Marital infidelity
- Multiple children
- Poor legal sanctions or enforcement of laws
- Poor parenting
- Pregnancy
- Psychiatric history
- The use and abuse of alcohol and drugs are strongly associated with a high probability of violence. Alcohol abuse is known to be a strong predictor of acute injury.
- Unemployment
Abuse usually begins with emotional or verbal threats and may escalate to physical violence. Victims of child abuse live in a constant state of fear. 11 Often, the abuser can become explosively violent. After the violent event, the abuser may apologize. This cycle usually repeats in child abuse. No matter the underlying circumstances, nothing justifies child abuse. Understanding the causes assists in understanding the behavior of an abuser. The abuser must be separated from the potential victim and treated for destructive behavior before a major event negatively impacts the lives of all involved.
Mandated reporters are required by law to all the SCR when while in their professional role, they develop a reasonable cause to suspect a child under the age of 18 is being maltreated or abused by a parent or person over the age of 18 who is legally responsible for the care of the child at that time.
Professional Role
The term “professional role” describes working or volunteering in a role that requires specific licensure or certification. Reasonable cause to suspect occurs when a mandated reporter observes or is told, in addition to professional experience or training, reasonably believes that a child has been or is being maltreated or abused. Reasonable suspicion does not require proof that a child has been maltreated or abused. Poverty in and of itself is not an indication of maltreatment or abuse.
Person Legally Responsible
The term “person legally responsible” (PLR) includes the child’s custodian, guardian, and any person responsible for the child’s care at the relevant time.
Confidentiality
- New York State law provides confidentiality to those who make a report.
- OCFS and the local CPS are not permitted to release to the subject of the report any data that would identify the source of the report, unless the reporter has given written permission for OCFS or CPS to do so. Information regarding the report source may be shared by OCFS or the local CPS with certain individuals (courts, police, district attorney), but only as provided by law.
- For more information on when the identify of a source of a report to the SCR may be disclosed, the mandated reporter can visit https://nysmandatedreporter.org.
- The mandated reporters legal obligation to report suspected child abuse and maltreatment supersedes client-patient confidentiality provisions.
Immunity from Liability
No organization may require the mandated reporter to seek permission prior to making a report of suspected child maltreatment or neglect, and they cannot retaliate against the mandated reporter for making a report.
Some mandated reporters face a conflict between their legal obligation to report and their legal obligation to maintain client or patient confidentiality. Section 419 of the Social Service Law provides immunity from liability for mandated reporters. Mandated reporters are immune from any criminal or civil liability if the report was made in good faith, even if CPS finds no evidence of abuse or maltreatment. The good faith of such a person, official, or institution required to report is presumed. This means if a person accuses the mandated reporter of making a false report in bad faith, they must prove that they acted with gross negligence or willful misconduct. Any mandated reporter who fails to call the SCR why they have reasonable suspicion of child abuse or maltreatment may be subjected to criminal and civil liability. The mandated reporter may also be held civilly liable for any harm suffered by a child due to failure to call the SCR.
Parents and PLRs must provide the children with the minimum degree of care. This includes adequate:
- Basic dental care
- Clothing
- Food
- Medical care
- Mental health services
- Shelter
- Treatment for drug or alcohol misuse
- Education
- Parents must ensure that children are actively enrolled in school. However, actively enrolled does not equate to earning high grades, participating in activities, or having perfect attendance. Adequate education is measured by monitoring the conduct of the parent after considering efforts previously made by the school or CPS.
- Supervision
- There is no law in New York that dictates how old a child must be to be left alone. The ability of a child to stay home alone is made on a case-by-case basis, and at a minimum, a child must be able to respond to a potential emergency, and care for themself. A child who is allowed to stay home alone may care for themselves, but they may not have the necessary skills to supervise other children.
- No excessive corporal punishment
- New York State allows parents to use corporal punishment to discipline their children, but it cannot be excessive. Excessive corporal punishment includes:
- When a child does not have the mental capacity to understand the reasoning for the punishment.
- A less severe form of punishment is available.
- The punishment occurs as a result of the parent’s anger.
- The child receives bruises or injuries as a result of the punishment
- The period of punishment outlasts the child’s endurance.
- The mandated reporter should take into consideration the parent’s financial ability regarding the minimum degree of care for food, clothing, shelter and medical care, and whether or not financial assistance or other reasonable means was offered.
- New York State allows parents to use corporal punishment to discipline their children, but it cannot be excessive. Excessive corporal punishment includes:
- Maltreatment
- Under New York law, a child is maltreated when:
- A parent of PLR fails to provide the minimum degree of care and that failure results in impairment or imminent danger of impairment to the child’s mental, physical, or emotional condition. Actual impairment does not have to occur for a child to be considered maltreated.
- The parent or PLR causes a nonaccidental serious physical injury to the child.
- Poverty is not a condition of maltreatment.
- Under New York law, a child is maltreated when:
- Abuse
- In the State of New York, abuse of a child occurs when:
- A parent, PLR, or other responsible for a child inflicts harm that causes, or has the potential to cause serious injury, death, disfigurement, or loss of function of a body part.
- A parent or PLR commits, or allows someone else to commit a sex crime against a child.
- In the State of New York, abuse of a child occurs when:
National Statutes
Federal Child Abuse Prevention and Treatment Act (CAPTA):
- Each state has specific child abuse statues. Federal legislation provides guidelines for defining acts that constitute child abuse. The guidelines suggest that child abuse includes an act or failure to act that presents an imminent risk of serious harm. This includes any recent act or failure to act on the part of a parent or caretaker that results in death, physical or emotional harm, sexual abuse, or exploitation.
Joint Commission on Accreditation of Healthcare Organizations Requirements
- Victims of alleged child abuse or neglect have specialized needs during the assessment process. The Joint Commission requires hospitals to have policies for the identification, evaluation, management, and referral of victims. This includes:
- Safeguarding information and potential evidence that may be used in future actions as part of the legal process.
- Having policies and procedures that define responsibility for collecting these materials.
- Having policies that define activities and specify who is responsible for their implementation.
- Provide an opportunity for victims of domestic violence to obtain help.
Social Services Law and Article 10 of the Family Court Act
- The laws that guide New York Child Protective Services are Article 6, Title 6 of the Social Services Law and Article 10 of the Family Court Act, including:12
- Section 413 of the Social Service Law requires designated professionals to report to the SCR when they have reasonable cause to suspect that a child before them in their professional capacity has been abused or maltreated. Or, when there is reasonable cause to suspect that a child is an abused or maltreated child where the parent, guardian, custodian, or other person legally responsible for such child comes before them in their professional official capacity and states from personal knowledge, facts, conditions, or circumstances which, if correct, would render the child an abused or maltreated child, then they must report.
- Whenever such a person is required to report as a member of the staff of a medical or other public or private institution, school, facility, or agency, they must make the report as required by this title.
- Nothing in this section or title is intended to require more than one report from any institution, school, or agency.
- No retaliatory personnel action is allowed.
Penalties for Failure to Report
Mandated reporters are subject to serious consequences for failure to report.
- A mandated reporter who fails to report can be found guilty of a Class A misdemeanor. A Class A misdemeanor can result in a penalty of up to a year in jail, a fine of up to $1,000.00, or both. Additionally, failing to report may result in a lawsuit in civil court for monetary damages for any harm caused by the mandated reporter’s failure to make the report to the SCR, including wrongful death suits. No medical or other public or private institution, school, facility, or agency shall take any retaliatory personnel action against an employee who made a report to the SCR. No school, school official, childcare provider, foster care provider, residential care facility provider, hospital, medical institution provider, or mental health facility provider shall impose any conditions, including prior approval or prior notification, upon a member of their staff mandated to report suspected child abuse or maltreatment.
- Class A misdemeanor, which can result in a penalty of up to a year in jail, a fine of $1,000, or both.
- Additionally, failing to report may result in a lawsuit in Civil Court for monetary damages for any harm caused by the mandated reporter’s failure to make the report to the SCR, including wrongful death suits.
- Mandated Reporters must call the SCR to ensure immunity and to be protected from criminal and civil liability. If the mandated reporter calls the local county department of social services office or a law enforcement official, then that mandated reporter has not fulfilled their legal duty to report to the SCR.
Effective November 21, 2005, an amendment to SSL §415 requires mandated reporters who make a report that initiates an investigation of an allegation of child abuse or maltreatment to comply with all requests for records made by CPS relating to such report. The mandated reporter to whom the request is directed makes the determination of what information is essential. If CPS believes that the mandated reporter has additional essential information pertaining to the report, CPS should ask the mandated reporter for the additional records and attempt to come to agreement regarding any additional records. If CPS and the mandated reporter cannot come to agreement and CPS disagrees with the mandated reporter’s rationale for why the records are not relevant to the report, CPS may seek a court order pursuant to CPLR Article 31 and SSL §415 directing the mandated reporter to produce the essential information. The amendment to SSL §415 only applies to the records of the mandated reporter who made the report of suspected child abuse or maltreatment. Additionally, the records that CPS requests should be limited only to information that directly pertains to the report itself. The purpose of the inclusion of these records is to support a full investigation of allegations of child abuse or maltreatment. This language is not intended to be an expansion of a mandated reporter’s current obligation. Since the passage of the federal HIPAA, confusion has arisen regarding the obligation of a mandated reporter to provide copies of written records that underlie the report. The intent of the amendment to SSL 415 is to make clear that the mandated reporter’s obligation also extends to the provision of the records necessary to investigate the report, as has always been the case.
Materials included are:13
- Records relating to diagnosis, prognosis, or treatment.
- Clinical records of any patient or client.
- Written reports from mandated reporters shall be admissible in evidence in any proceedings relating to child abuse or maltreatment.
- The statutory amendments do not require written consent and are intended to promote CPS getting the needed supplemental information that supports the initial report.
Abandoned Infant Protection Act
The Abandoned Infant Protection Act (AIPA) does not affect responsibilities as a mandated reporter. The AIPA does not amend the law regarding mandated reporters and does not in any way change or lessen the responsibilities of mandated reporters. Mandated reporters who learn of abandonment are still obligated to fulfill their legal responsibility. The SCR only registers reports against a parent, guardian, or other person eighteen years of age or older who is legally responsible for the child. According to the Family Court Act, people legally responsible include the child’s custodian, guardian, and any other person 18-years old or older responsible for the child’s care at the relevant time. This includes any person continually or at regular intervals found in the same household as the child when the conduct of such person causes or contributes to the abuse or maltreatment of the child. Once the SCR registers a report, the person who is named as causing the harm to the child becomes the “subject of the report.” Teachers in most public or private schools do not qualify as “subjects of reports” when they are acting as teachers. Teachers can be “subjects of reports” when the incident involves their own child or with a child, they have legal responsibility for outside of their role as a teacher.
Only one report is required to be submitted, organizations are prohibited from retaliation against any employee making a report.
Identifying a child of suspected maltreatment and abuse is difficult because the child may be nonverbal or too frightened or severely injured to talk. Also, the perpetrator will rarely admit to the injury, and witnesses are uncommon. In a healthcare setting, healthcare providers will see children of abuse in a range of ways that include:4,12,13,24
- An adult or mandated reporter may bring the child in when they are concerned for abuse.
- A child or adolescent may come in disclosing the abuse.
- The perpetrators may be concerned that the abuse is severe and bring in the patient for medical care.
- The child may present for care unrelated to the abuse, and the abuse may be found incidentally.
Physical abuse should be considered in the evaluation of all injuries of children. A thorough history of present illness is important to make a correct diagnosis. Important aspects of the history-taking involve gathering information about the child’s behavior before, during, and after the injury occurs. History-taking should include interviewing the verbal child and each caretaker separately. The verbal child and parent or caretaker should be able to provide their history without interruptions in order not to be influenced by the healthcare provider’s questions or interpretations.
Abusive Head Trauma
Abusive head trauma (AHT), also known as the shaken baby syndrome (SBS), is a preventable, severe form of physical child abuse resulting from violently shaking an infant or toddler by the shoulders, arms, or legs. Shaken baby syndrome and the resultant head injury has leading cause of death related to child abuse; nearly 25%.6,7,810 Symptoms may be as subtle as vomiting, or as severe as lethargy, seizures, apnea, or coma. Findings suggestive of AHT are retinal hemorrhages, subdural hematomas, and diffuse axonal injury. 6,7,810 An infant with abusive head trauma may have no neurologic symptoms and may be diagnosed instead with acute gastroenteritis, otitis media, GERD, colic, and other non-related entities. Often, a head ultrasound is used as the initial evaluation in young infants. However, it is not the test of choice in an emergency setting. In the assessment of AHT, the ophthalmologic examination should be performed, preferably by a pediatric ophthalmologist. The injuries seen in infants and toddlers with Abusive Head Trauma (AHT) may include:6,7,810
- Bleeding on the back surface of the eyes (retinal hemorrhages).
- Bleeding over the surface of the brain (subdural hemorrhages).
- Other brain injuries, including brain swelling and injuries to the white matter of the brain.
- Some victims have evidence of blunt impact to the head; others do not.
- Some victims have other evidence of physical abuse, including bruises, abdominal injuries, and recent or healing broken bones; others do not.
Nearly all victims of AHT suffer serious, long-term health consequences. Examples include:
- Developmental Delays
- Hearing Loss
- Physical Disabilities
- Vision Problems
It is the responsibility of every healthcare provider to play a role in preventing abusive head trauma. They must know the risk factors and the triggers for abuse, inform and teach the parent or caregiver the dangers of shaking or hitting a baby’s head, and identify support for the parents and caregivers in their community.
When teaching the parent or caregiver about abusive head trauma, it is imperative that the healthcare provider ensures that the parent or caregiver:
- Understands that infant crying is worse in the first few months of life but will get better as the child grows.
- Understands that soothing a crying baby is not easy, but they can calm the baby by breastfeeding, offering a bottle or pacifier, singing, swaddling, taking the baby for a ride in the car or walk in the stroller, laying the baby across their lap on the baby’s stomach and gently rubbing or patting the baby’s back.
- Calls a friend or relative, or uses a parent helpline for support.
- Check for signs of illness and call the doctor if the child appears to be sick and will not stop crying.
- Never leaves the baby with a person who is easily irritated, has a temper, or has a history of violence.
Abdominal Trauma
Abdominal trauma is a significant cause of morbidity and mortality in abused children. 13,24 It is the second most common cause of death from physical abuse and is mostly seen in infants and toddlers. Many of these children will not display overt findings, and there may be no abdominal bruising on physical exam. 13,24 Therefore, screening should include liver function tests, amylase, lipase, and testing for hematuria. Any positive result can indicate the need for imaging studies, particularly an abdominal computerized tomography (CT) scan.
Skeletal Trauma
The second most common type of child abuse after neglect is physical abuse. 13,24 Eighty percent of abusive fractures occur in non-ambulatory children, particularly in children younger than 18 months of age. 13,24 The most important risk factor for abusive skeletal injury is age. There is no fracture pathognomonic for abuse, but there are some fractures that are more suggestive of abuse. These include posterior or lateral rib fractures and “corner” or “bucket handle” fractures, which occur at the ends of long bones, and which result from a twisting mechanism. Other highly suspicious fractures are sternal, spinal, and scapular fractures.
Neglect
A physical examination may not only demonstrate signs of physical abuse but may show signs of neglect.13,24 A general examination may show poor oral hygiene with extensive dental caries, malnutrition with significant growth failure, untreated diaper dermatitis, or untreated wounds.
All mandated reporters are required to make a report to the SCR when there is a reasonable suspicion of abuse or neglect.13,24 The mandated reporter does not need to be certain of child abuse to report it; they just must have a reasonable suspicion that it is occurring. This mandated report may be lifesaving for many children.
Physical Abuse
Child physical abuse should be considered in each of the following: 1,3,4
- A non-ambulatory infant with any injury.
- A statement of harm from the verbal child.
- Behavior changes; including
- Child not acting like they normally do, acting shy, or attention seeking.
- Changes in school performance and activities
- Self-destructive behavior
- Exhibit isolation
- Begging or stealing food
- Showing reluctance to go home
- Alcohol use
- Illicit drug use
- Multiple school absences
- Showing knowledge of sexual behavior that is inconsistent with the child’s age.
- Bruises on the torso, ear, or neck in a child younger than 4 years of age.
- Bruises or lacerations shaped like an object.
- Burns to genitalia.
- Inconsistencies or discrepancies in the history provided by the parent or caregiver.
- Injury in a nonverbal child.
- Injury is inconsistent with child’s physical abilities; the location is atypical, and the explanation does not match the pattern of injury.
- Mechanism of injury not plausible; multiple injuries, particularly at varying stages of healing.
- Pain/itching in genital area
- Physical development or growth delays
- Stocking or glove injury distributions or patterns.
- The parent or caregiver is unconcerned about the injury.
- There is an unexplained delay in seeking care.
“TEN 4” is a useful mnemonic device used to recall which bruising locations are of concern in cases involving physical abuse: Torso, Ear, Neck and 4 (less than four years of age or any bruising in a child less than four months of age). A few injuries that are highly suggestive of abuse include retinal hemorrhages, posterior rib fractures, and classic metaphyseal lesions.
Bruising is the most common sign of physical abuse but is often missed as a sentinel injury in ambulatory children. Bruising in non-ambulatory children is rare and should raise suspicion of abuse. The most common areas of bruising in non-abused children are the knees and shins as well as bony prominences including the forehead. The most common area of bruising for the abused children includes the head and face. Burns are a common form of a childhood injury that is usually not associated with abuse. Immersion burns have characteristic sharp lines of demarcation that often involves the genitals and lower extremities in a symmetric pattern, and this is highly suspicious for abuse.
Sexual Abuse
About 25% of girls and 8% of boys will experience child sexual abuse at some point in childhood, and 91% of the abuse is perpetrated by someone the child or child’s family knows. Sexual abuse can affect how a child behaves, thinks, and feels over a lifetime. 2,9,21 This can cause short and long-term emotional, behavioral, and physical health consequences. These consequences include: 21,22, 23
- Chronic health conditions later in life
- Depression
- Increased risk for suicide or suicide attempts
- Physical injuries
- Posttraumatic stress disorder (PTSD)
- Risky sexual behaviors
- Substance abuse
- Unwanted/unplanned pregnancies
Another outcome commonly associated with child sexual abuse is an increased risk of re-victimization throughout a person’s life.22 If a child demonstrates behavior such as undressing in front of others, touching others’ genitals, as well as trying to look at others underdressing, there may be a concern for sexual abuse. It is important to understand that a normal physical examination does not rule out sexual abuse. In fact, most sexual abuse victims have a normal anogenital examination. In most cases, the strongest evidence that sexual abuse has occurred is the child’s statement.
Children who are abused may be unkept and/or malnourished, and may also display inappropriate behavior such as aggression, being withdrawn, and have poor communication skills. Others may be disruptive or hyperactive. They also may have poor school attendance.
Specific injuries and associated findings of child abuse include: 15
| Bites | Chipped teeth |
| Cigarette or cigar burns | Craniofacial and neck injuries |
| Friction burns | Injuries at different stages of healing |
| Injuries to multiple organs | Intracranial hemorrhage |
| Long-bone fractures | Marks shaped like belt buckles and cords |
| Oral burns, contusions, or cuts | Patterned injuries |
| Poor dental health | Sexually transmitted diseases |
| Skull fractures | Strangulation injuries |
| Unusual injuries |
When considering child abuse, one must also consider health conditions that may coincide with injuries. The health conditions may include: 15
Head Trauma
| Accidental injury | Arteriovenous malformations |
| Bacterial meningitis | Birth trauma |
| Cerebral sinovenous thrombosis | Hemophilia |
| Leukemia | Neonatal alloimmune thrombocytopenia |
| Metabolic diseases | Solid brain tumors |
| Unintentional asphyxia |
Bruises and Contusions
| Accidental bruises | Birth trauma |
| Bleeding disorder | Coining |
| Cupping | Congenital dermal melanocytosis (Mongolian spots) |
| Erythema multiforme | Hemangioma |
| Hemophilia | Hemorrhagic disease |
| Henoch-Schonlein purpura | Idiopathic thrombocytopenic purpura |
| Insect Bites | Malignancy |
| Nevi | Phytophotodermatitis |
| Subconjunctival hemorrhage from vomiting or coughing |
Burns
| Accidental burns | Atopic dermatitis |
| Contact dermatitis | Impetigo |
| Inflammatory skin conditions | Sunburn |
Fractures
| Accidental | Birth trauma |
| Bone fragility with chronic disease | Caffey disease |
| Congenital syphilis | Hypervitaminosis A |
| Malignancy | Osteogenesis imperfecta |
| Osteomyelitis | Osteopenia |
| Osteopenia of prematurity | Physiological subperiosteal new bone |
| Rickets | Scurvy |
When child abuse or maltreatment is suspected, the indicators should never be viewed in isolation. The indicator for abuse and maltreatment should be considered in relation to the child’s age, circumstances, and their physical condition and behavior. Abuse or maltreatment should never be assumed, rather the mandated reporter should listen, and try to understand any explanation provided for the presenting concern, and asses whether the explanation is consistent with the physical injuries or behaviors.
Intellectual and developmental disabilities (IDDs) are disorders that are usually present at birth and that negatively affect the trajectory of a child’s physical, intellectual, and/or emotional development. Many of these conditions affect multiple body parts or systems.25
Intellectual disability begins any time before the age of 18 and is characterized by differences with intellectual functioning or intelligence, and adaptive behavior.
- Intellectual functioning or intelligence includes the ability to learn, reason, and problem solve.
- Adaptive behavior includes everyday social and life skills.
Intellectual and developmental disabilities is the term often used to describe situations in which intellectual disability and other disabilities are present.The IDDs can be reviewedin regards to how they occur, or the body parts or systems they affect, such as:
- Nervous system
These disorders affect how the brain, spinal cord, and nervous system function, which can affect intelligence and learning. These conditions can also cause other issues, such as behavioral disorders, , seizures, speech or language difficulties, and trouble with movement. The following are examples of IDD conditions related to the nervous system: 25- Cerebral palsy – A group of movement disorders that appear in early childhood. Signs and symptoms vary among people and over time, but include poor coordination, stiff, weak muscles and tremors.
- Down syndrome – A genetic condition caused when an unusual cell division results in an extra full or partial copy of chromosome 21. This extra genetic material causes developmental changes and physical features
- Fragile X syndrome – Also known as Martin-Bell syndrome, is a genetic condition that affects a child’s learning, behavior, appearance, and health.
- Autism spectrum disorder (ASD) – Neurological and developmental disorders that affect how people behave, communicate, learn, and interact with others. Although autism can be diagnosed at any age, it is described as a developmental disorder because symptoms generally appear in the first two years of life.
- Familial dysautonomia – Also known as Riley–Day syndrome, is a rare, progressive, recessive genetic disorder of the autonomic nervous system that affects the development and survival of sensory, sympathetic, and some parasympathetic neurons in the autonomic and sensory nervous system.
- Prader-Willi syndrome – A rare genetic condition that affects a child’s metabolism and causes changes to their body and behavior. They have severe low muscle tone and poor feeding during early infancy, followed by a tremendous appetite that develops between 2 and 6 years of age. This can lead to severe obesity if excessive eating isn’t managed.
- Neurological impairment – Conditions that affect the nervous system, leading to disruptions in movement, cognition, and overall functioning.
- Sensory system
Disorders that affect the senses (hearing, sight, smell, taste, and touch) or how the brain processes or interprets information from the senses. For instance, infants exposed to infections, such as cytomegalovirus, may have reduced function with their eyesight and/or hearing. In addition, being touched or held can be difficult for people with ASDs. - Metabolism
Disorders that affect how the body uses food and other materials for energy and growth. For example, how the body breaks down food during digestion is a metabolic process. Phenylketonuria (PKU) and congenital hypothyroidism are examples of metabolic conditions that can lead to IDDs. - Degenerative
Individuals with degenerative disorders may seem to be typical at birth and may initially meet the usual developmental milestones, but over time they will experience disruptions in abilities, functions, and skills. Some degenerative disorders result from other conditions, such as untreated problems of metabolism.
Physical Indicators of Abuse and Neglect in Children with Intellectual Disabilities
Indicators of abuse and neglect in children with intellectual disabilities are often like those in other children, but they can be easily overlooked or explained away. In many cases, a mandated reporter may attribute injuries to accidents caused by the child’s disability or even to self-harm. It is critical to distinguish between genuine accidental injuries and suspicious signs of maltreatment or abuse. Signs of maltreatment and abuse may include:25
- Bruises and Marks in Unusual Places
Bruising is one of the most common signs of physical abuse. Bruises may be in locations that are not typical for childhood play injuries, such as the upper arms, back, thighs, or genital area, or bruises in specific shapes, like the outline of a hand or belt. There also may be multiple bruises in clusters or of varying ages.
- Frequent or Unexplained Injuries
Patterns of cuts, burns, or fractures can indicate abuse. Burns in shapes, like a cigarette tip or hot water immersion line are red flags. Also, frequent ER visits for injuries or accidents should raise concern.
- Restraint or Harsh Handling
Grip marks on arms or chest, which could indicate grabbing or shaking, ligature or rope marks on wrists or ankles, or abrasions that suggest the child was tied or gagged may indicate abuse. Petechiae (tiny red spots from broken blood vessels) on the face or neck may be the result of choking or strangulation attempts.
- Dental and Facial Injuries
Broken teeth, facial bruises, or torn frenulum (the small piece of tissue under the lip or tongue) can indicate force feeding or blows to the mouth. Children with intellectual disabilities might not be seen regularly by a dentist, so dental injuries or untreated cavities can go unnoticed for long periods.
- Signs of Sexual Abuse
Though often hidden, physical signs of sexual abuse can include difficulty walking or sitting, bruises or bleeding in the genital or anal areas, recurrent urinary tract infections, or sexually transmitted infections. Incontinence in a child who was previously toilet-trained or sudden fear of toileting can also be indicators.
- Poor Hygiene and Unattended Medical Needs
A neglected child may appear consistently unkempt, with infrequent bathing, persistent diaper rash, or clothes soiled with urine or feces. Overgrown hair and nails, skin infections, or severe dental decay are common in neglect. For children with IDD who rely on caregivers for personal care, neglect may manifest as pressure sores or untreated health issues.
- Malnutrition and Weight Issues
Consistent hunger, obvious weight loss, or malnourishment can indicate that a child is not being fed adequately. A child who is constantly thirsty, begs for food, or is significantly underweight should prompt questions about whether their nutritional needs are met.
- Lack of Supervision and Unsafe Environments
Neglect may involve leaving a child with IDD unsupervised or in hazardous conditions. Signs can include frequent accidents or injuries because no one was watching the child. The home environment might have dangers like accessible poisons, sharp objects, or lack basic safety accommodations.
Behavioral and Emotional Indicators of Child Maltreatment and Abuse in Children with IDD
Children with limited verbal abilities often communicate distress through their behavior and emotions. In children with IDD, behavioral and emotional signs may be the primary clues to underlying abuse or neglect. The signs may include:25
- Sudden Changes in Behavior
Any unexplained change in behavior or personality can be a red flag. For instance, a generally active child may become withdrawn, or normally friendly child may become aggressive. In children with IDD, a sudden onset of tantrums, self-harm such as head-banging or biting, or destructiveness such as breaking toys may signal trauma.
- Extreme Emotional Reactions
Noticeable shifts in mood such as frequent crying spells, depression, or intense anxiety may indicate abuse. A child who was once relatively calm may develop mood swings, panic attacks, or phobias without obvious cause.
- Regression or Loss of Skills
Maltreatment or abuse can cause some children to regress developmentally. A child may lose skills or independence they had previously mastered. For example, a potty-trained child might start bed-wetting, or one who could feed themselves may suddenly seem helpless.
- Withdrawal and Isolation
A child who was once social may withdraw from interactions, avoid eye contact, or hide away to cope with abuse or maltreatment.
- Heightened Aggression or Irritability
Some children may react to abuse with anger and aggression. A child with IDD who experiences trauma related to maltreatment or abuse may have increased aggression, irritability, or frequent outbursts and lash out at siblings, peers, or caregivers.
- Nightmares and Sleep Problems
Children who have been abused often develop nightmares, night terrors, or insomnia. A child may suddenly fear the dark or resist going to bed.
Communication Barriers
Many children with IDD have limited verbal skills or alternative ways of communicating. They may have speech impairments, be non-verbal, or have limited understanding of vocabulary, making it difficult for them to disclose maltreatment or abuse. Some children may only be able to communicate through simple speech, behaviors, or simple signals, which can be misunderstood, as adults may not comprehend what they are trying to communicate.
Young children or those with more severe intellectual impairments may express their experiences of abuse or maltreatment through play or repetitive stories by repeatedly acting out scenes of violence with dolls or using explicit sexual language beyond their developmental level. An infographic summarizing key signs of trauma in children with intellectual or developmental disabilities, such as behavioral changes (aggression, irritability, or withdrawal), physical symptoms (headaches or sleep problems), and trauma-themed repetitive play can all signal that a child with IDD has experienced abuse, maltreatment, or distress. Increases in difficulty with everyday skills and cognitive issues (memory or learning problems) after a trauma are also noted as potential indicators. 25
Concerning Behavioral Indicators of Caregivers to Children with IDD:
- Appears to be indifferent to the child
- Behaves irrationally or in a bizarre manner
- Constantly blaming, belittles, or berates the child
- Demands a level of physical or academic performance the child cannot achieve.
- Has a history of abuse as a child
- Has a history of abusing animals or pets
- Is abusing alcohol or other drugs
- Is unconcerned about the child and refuses to consider offers of help for the child’s problems.
- Looks primarily to the child for care, attention, and satisfaction of the parent’s emotional needs.
- Offers conflicting, unconvincing, or no explanation for the child’s injury, or provides an explanation that is inconsistent with the injury.
- Overtly rejects the child
- Seems apathetic or depressed
- Sees the child as entirely bad, worthless, or burdensome
- Shows little concern for the child
- Uses harsh physical discipline with the child or asks teachers or other caregivers to use harsh physical discipline.
One of the biggest challenges in identifying physical abuse in children with IDD is the tendency to rationalize injuries or conditions as being caused by the disability or the child’s own behaviors.25 For example, if a child with autism has bruises, a mandated reporter may assume the child caused the injuries themself or that the child has poor motor coordination. It is true that some children with IDD do engage in behaviors like head-banging or scratching that can cause marks, however, it is crucial to carefully assess the pattern and explanation of any injury. Even if a child has a known self-harming behavior or medical condition that could explain an injury, abuse or maltreatment should still be considered and ruled out. It is better to investigate and ensure the injury was accidental than to miss a pattern of abuse. 25
Another commonly overlooked situation is when a child’s disability masks neglect. A caregiver may claim that a child is refusing to eat, or has a rash because of a medical condition, shifting the blame of the situation to the child’s disability. While children with IDD can have difficulties feeding or sensitive skin, caregivers are responsible for managing these issues. Prolonged poor hygiene, untreated ailments, or underweight conditions are not normal parts of any disability; they are signs that the caregiver is failing to meet the child’s basic needs. Sadly, a child with an intellectual disability may not realize that their situation is abnormal or may not know how to seek help. This is why external observation of physical signs is vital.25
Mandated reporters may have interactions with children that occur in a virtual environment. For example, children may experience telehealth with a healthcare provider, participate in online therapy, or attend school remotely. When interacting with children while in their professional role, mandated reporters are obligated to the same level of responsibilities in the virtual environment as mandated reporters who interact with children in person.
When assessing safety virtually, the mandated reporter should:12
- Be alert for indications that a child is trying to communicate something without someone else in the room noticing.
- Note if a child’s demeanor or behavior is different when someone else enters the room.
- Listen for concerning statements a child makes to siblings, their peers, or to you.
- Try to observe the child’s body, even if only the child’s face, neck, shoulders, and chest are visible, for any signs of abuse.
- Assess the child’s mood and demeanor (appearance of anxiousness or depression).
In the virtual environment, a mandated reporter may observe or hear an altercation between children or adults. If what is heard or observed does not rise to a level of making a report, it may still create an opportunity for a conversation about safety or managing stress.
Mandated reporters should always use reliable technology with adequate lighting and sound when communicating with children or their family members. At the start of each visit, the child’s location should be verified in case emergency services are needed. All members in the virtual environment should be introduced at the beginning of the virtual visit, and whenever someone enters after the visit begins. The child or family member should be asked if there is sufficient privacy to discuss sensitive matters. If there is not enough privacy, household members who are not participating in the virtual visit should be asked to leave the area, if possible. The child should be present for at least part of the visit.12
During the visit, nonverbal cues should be monitored and noted. If a child’s demeanor or behavior changes when someone else enters the room, this should prompt further exploration. For instance, if a child turns off a webcam or is very hesitant to use one when someone else is present, this can be a sign that they are trying to avoid confrontation or visual assessment.12
In addition, the mandated reporter should monitor the child’s environment for noticeable unsafe conditions. It should be clear that there is appropriate supervision for the child, and that young children are not watching over younger siblings.
Prior to the end of the virtual visit, all mandated reporters who have virtual contact with a child should provide clear channels of communication through chat, email, phone, text, or online tools.
Educational Neglect
Poor school attendance does not equate to a reasonable cause to suspect maltreatment of a child. School personnel should first try working with the child, family, and community agencies to identify needs and resources available. If unsuccessful, a report of suspected educational neglect should be called in to the SCR as a remedy for excessive absences only as a last resort.
To warrant a report to the SCR for educational neglect, all of the following elements must be present:12
- No parent or responsible person has taken any action to rectify the situation.
- Child must be of compulsory school age and currently living in New York State.
- Child must be excessively absent without a valid reason or excuse.
- The child’s education must be impaired due to the excessive absenteeism (or the child has an IEP and has missed necessary services due to excessive absenteeism).
- The parent or responsible person has been made aware of the excessive absenteeism and impairment by means beyond simply sending a note home or leaving a voicemail message.
- School officials have made efforts to engage the child and parent/responsible person.
Exercise
Octavia has presented to the healthcare clinic with her 13 year old daughter. Mandy, Octavia’s 13 year old daughter, is complaining of abdominal pain. Upon meeting Octavia and Mandy, Octavia appears frustrated, and complains to you about the long wait time. She also complains of being away from home, and making her boyfriend miss work to watch her other children while she and Mandy are at the clinic. Mandy states that she has had stomach pain before, but the most recent episode is ongoing, and the cramping pain is located in her lower abdomen. Octavia also offers information that Mandy started her menstruation 3 months ago, that she thinks her menstruation is due, and questions whether the pain can be associated with the onset of menstruation. Octavia also mentions recent changes in Mandy’s behavior at home, but suggests it is related to “being a teenager”. When observing the interaction between Octavia and Mandy, you notice that Mandy does not make eye contact with her mother, guards her stomach, and winces whenever her mother moves her arms. You inform the mother that you will need to assess Mandy, and then ask Mandy if it is OK to perform a physical examination on her. Mandy begins to cry, and yells at her mother “I know why it hursts, and so do you!” Octavia becomes upset, grabs Mandy’s arm, and tries to force her to walk out of the clinic area. You suspect that Mandy may be a victim of abuse. What are your next steps?
Answer
If while in your professional role, and as a mandated reporter you have a reasonable suspicion that a child is being abused or maltreated, you are required to call the SCR immediately on the mandated reporter designated hotline at 1-800-635-1522. You should always call 911 first if in an emergency situation. As a mandated reporter, you should use the LDSS-2221A form to gather information, and then use it as a tool to organize the information while making the call. Information needed to complete the form includes:
- Full name of the parent or person legally responsible for the child.
- Parents or other adults’ dates of birth, when available.
- Full name of the child or children you suspect are being abused or maltreated.
- Child or children’s dates of birth, when available.
- Specific information which led to you having a reasonable suspicion of abuse or maltreatment.
- Addresses or locating information for the relevant adults and children – Please note that it is crucial that you have an address or locating information for the child and/or relevant adults when you call the SCR. The SCR will not be able to accept the report if you do not have this information.
- Your full name as Mandated Reporter .
- The name of your agency or organization.
- Your contact information including phone number and email address.
- The name of any other mandated reporter you believe personally observed or was provided with relevant information about the child.
After you complete the call to the SCR, you must immediately notify the person in charge of the institution, school, facility, or agency, or the designated agent of the person in charge, and provide the information reported to the SCR, including the names of other persons identified as having direct knowledge of the alleged abuse or maltreatment and other mandated reporters identified as having reasonable cause to suspect.
If while in their professional role, a mandated reporter has a reasonable suspicion that a child is being abused or maltreated, they are required to call the SCR immediately on the mandated reporter designated hotline at 1-800-635-1522. They should always call 911 first if in an emergency situation.
If a mandated reporter is not acting in their official capacity when the call is made, then they must call the non-mandated reporter hotline phone number at 1-800-342-3720.
Two counties in New York State have their own localized hotlines that may be used instead of the SCR hotline.
Onondaga County (315)-422-9701
Monroe County (585)-461-5690
| New York State Office of Children and Family Services 518-473-7793 https://www.ocfs.state.ny.us/main/ Prevent Child Abuse New York Helpline English and Spanish 800-342-7472 – 24 hrs. www.preventchildabuseny.org New York State Domestic Violence Hotline 800-942-6906 English 800-942-6908 Spanish www.opdv.state.ny.us |
(LDSS 2221-A)
The mandated reporter should use the LDSS-2221A form to gather information, and then use it as a tool to organize the information while making the call. Form is available on OCFS’ website: https://ocfs.ny.gov/forms/ldss/LDSS-2221/OCFS-LDSS-2221A.docx
Information needed to complete the form includes:
- Full name of the parent or person legally responsible for the child.
- Parents or other adults’ dates of birth, when available.
- Full name of the child or children you suspect are being abused or maltreated.
- Child or children’s dates of birth, when available.
- Specific information which led to you having a reasonable suspicion of abuse or maltreatment.
- Addresses or locating information for the relevant adults and children – Please note that it is crucial that you have an address or locating information for the child and/or relevant adults when you call the SCR. The SCR will not be able to accept the report if you do not have this information.
- Your full name as Mandated Reporter.
- The name of your agency or organization.
- Your contact information, including phone number and email address.
- The name of any other mandated reporter you believe personally observed or was provided with relevant information about the child.
Upon completion of the form, the mandated reporter must send the LDSS-2221A form to their Local Department of Social Services. There is a link included on the form to assist with finding that address.
The SCR is bound by legal criteria which dictate whether they can accept a report. The following 3 criteria must be met for the SCR to accept a report:
- The child must be born and under 18 years of age.
- The alleged perpetrator must be the child’s parent or over age 18 and the PLR.
- The conduct must meet the legal definition for maltreatment or abuse.
The SCR is not legally required to accept a report simply because a mandated reporter makes a call. The SCR staff will conduct their own interview to determine if the information provided by the mandated reporter rises to the legal level of suspected child abuse or maltreatment.
If the SCR accepts the report, the mandated reporter should write down the call identification (ID) number given by the CPS Specialist at the SCR. On the upper right corner of the 2221A there is a place to record the call ID number. Two copies of the form, an original and a duplicate must be forwarded to the local CPS agency within 48 hours. A third copy should be kept on file by the reporter.
When the circumstances of the mandated reporter’s call to the SCR constitute a crime or an immediate threat to the child’s health or safety, but the report is not registerable, the SCR will send the information to the New York State Police Information Network (NYSPIN), or to the New York City Police Department (NYPD) for necessary action.
These types of calls are referred to as Law Enforcement Referrals, or “LERs.” They are transmitted to the appropriate police agency for follow-up. They are not registered SCR reports. LERs are not assigned a call identification number. If the mandated reporter is in a LER situation, they do not need to complete the LDSS-2221A form.
After the mandated reporter completes their call to the SCR, they must immediately notify the person in charge of the institution, school, facility, or agency, or the designated agent of the person in charge, and provide the information reported to the SCR, including the names of other persons identified as having direct knowledge of the alleged abuse or maltreatment and other mandated reporters identified as having reasonable cause to suspect.
The person in charge or designated agent, once notified that a report has been made to the SCR, becomes responsible for all subsequent administration concerning the report.
As suggested earlier, if time permits, it may be helpful for the mandated reporter to fill out the form before placing their call to the SCR. This enables them to organize whatever demographic and identifying information they may have, as well as their allegations and concerns. The safety of the child must come before the completion of the form.
Written reports, using the LDSS-2221A, should be sent to the local CPS office within 48 hours of making the oral report. Once the local department of social services receives the report they must initiate an investigation within 24 hours. During the investigation, the assigned CPS caseworker must comply with numerous regulations and policies to ensure they conduct a thorough investigation and safety assessment. They are also required to contact the parent or PLR and child(ren) involved, contact the source of the report, and request copies of records or reports, which by law, must be provided.
Within 60 days, the CPS agency must determine whether the allegations are substantiated (meaning there was a fair preponderance of evidence the allegations were true) or unsubstantiated (meaning there was not a fair preponderance of evidence the allegations were true). The most common outcome of a CPS investigation is that the caseworker will work with the family to obtain necessary services or aid to alleviate problems and promote safety. It is important to keep in mind that CPS intervention is not required for parents, children, or families to obtain services, and mandated reporters can support a family without having to make a report.
Special Considerations
In a healthcare setting, when feasible and without delaying care to a child, and guided by institutional policies, photographs of injuries should be taken prior to initiating treatment of suspected injuries of child abuse.
- Check photos as they may be used in court.
- Take an identification tag photo.
- Take photos from multiple injury angles and distances.
- Measure and document injury sizes.
- When photographing bite marks include photos focusing on each dental arch to avoid distortion.
Child abuse is a public health problem that leads to lifelong health consequences, both physically and psychologically. Physically, children who are victims of abusive head trauma may have neurologic deficits, developmental delays, cerebral palsy, and other forms of disability. Psychologically, victims of child abuse tend to have higher rates of depression, conduct disorder, and substance abuse. Academically, these children may have poor performance at school with decreased cognitive function. It is important for healthcare providers to have a high index of suspicion for child abuse because early identification may be lifesaving. All healthcare providers should report child abuse without hesitation.
When it comes to child abuse, all mandated reporters have a legal, medical, and moral obligation to identify the suspected abuse and report it to child protective services. Many child abuse victims present to health institutions, and healthcare providers are often the first ones to suspect abuse. The key is to be aware of signs of abuse. Allowing abused children to return to their perpetrators usually leads to more violence, and sometimes even death. Even if child abuse is only suspected, the healthcare provider must notify the appropriate personnel and agencies. The law favors the healthcare provider for reporting child abuse, even if it is only a suspicion. On the other hand, failing to report child abuse can have repercussions on the mandated reporter, including litigation and incarceration. The mandated reporter should use the LDSS-2221A form to gather information, and then use it as a tool to organize the information of the abuse while making the call.
If the Statewide Central Register (SCR) of Abuse and Maltreatment accepts the report, the mandated reporter should write down the call identification number given by the Child Protective Services (CPS) Specialist at the SCR. On the upper right corner of the 2221A there is a place to record the call identification number (ID). Two copies of the form, an original and a duplicate must be forwarded to the local CPS agency within 48 hours. A third copy should be kept on file by the reporter.
New York State Reporting Center Phone Numbers
State Central Register for Child Abuse and Maltreatment
Mandated Reporter Telephone Number 1-800-635-1522. Use this number when reporting suspicions within your professional capacity.
Non-Mandated Telephone Number 1-800-342-3720. Use this number when reporting suspicions outside your professional capacity.
People in Monroe County may call a local reporting number: 1-585-461-5690
People in Onondaga County may call a local reporting number: 1-315-422-9701
New York State Office of Children and Family Services
518-473-7793
https://www.ocfs.state.ny.us/main/
Prevent Child Abuse New York Helpline
English and Spanish
800-342-7472 – 24 hrs.
New York State Domestic Violence Hotline
800-942-6906 English
800-942-6908 Spanish
Steps to Report Suspected Child Abuse
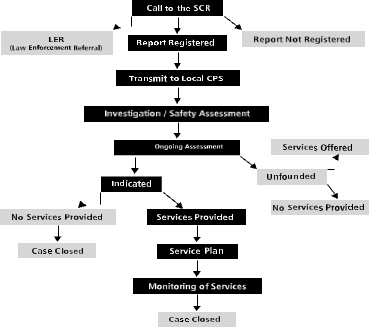
New York State is divided into fifty-eight local social services districts. The five boroughs of New York City comprise one district. Outside of New York City each district corresponds to one of the fifty-seven counties that make up the remainder of the state. County Departments of Social Services (DSS) provide or administer the full range of publicly funded social services and cash assistance programs. Families whose income meets state guidelines and who meet other criteria, may be able to receive a subsidy to offset some of their childcare costs. Listed below is an alphabetical list of the fifty-eight DSS Offices available throughout New York State.
Albany County DSS
162 Washington Avenue Albany, NY 12210 (518) 447-7300 Website: https://www.albanycounty.com/departments/dss/
Allegany County DSS
County Office Building ·7 Court St. · Belmont, NY 14813-1077 (585) 268-9622 Website: https://www.alleganyco.com/default.asp?show=btn_dss
Broome County DSS
36-42 Main Street · Binghamton, NY 13905-3199
(607) 778-8850 Website: https://www.gobroomecounty.com/dss/
Cattaraugus County DSS
One Leo Moss Drive · Suite 6010 · Olean, NY 14760-1158 (716) 373-8065 Website: https://www.co.cattaraugus.ny.us/dss/
Cayuga County DSS
County Office Building · 160 Genesee Street · 2nd Floor · Auburn, NY 13021-3433 (315) 253-1011 Website: https://co.cayuga.ny.us/hhs/index.html
Chautauqua County DSS
Hall R. Clothier Building · Mayville, NY 14757 (716) 753-4421 Website: https://www.co.chautauqua.ny.us/hservframe.htm
Chemung County DSS
Human Resource Center · 425 Pennsylvania Avenue · Elmira, NY 14902· (607) 737-5309
Chenango County DSS
5 Court Street · Norwich, NY 13815 · (607) 337-1500
Clinton County DSS
13 Durkee Street · Plattsburgh, NY 12901-2911· (518) 565-3300 Website: https://www.clintoncountygov.com/Departments/DSS/index.htm
Columbia County DSS
25 Railroad Avenue · P.O. Box 458 · Hudson, NY 12534 · (518) 828-9411
Cortland County DSS
County Office Building· 60 Central Avenue · Cortland, NY 13045-5590 · (607) 753-5248 Website: https://www.cortland-co.org/dss/
Delaware County DSS
111 Main Street · P.O. Box 469 · Delhi, NY 13753-1265· (607) 746-2325
Dutchess County DSS
60 Market Street · Poughkeepsie, NY 12601-3299· (845) 486-3000
Website: https://www.co.dutchess.ny.us/CountyGov/Departments/SocialServices/SSIndex.htm
Erie County DSS
Rath County Office Building · 95 Franklin Street, 8th Floor · Buffalo, NY 14202-3959 · (716) 858-8000 Website: https://www.erie.gov/depts/socialservices/
Essex County DSS
7551 Court St.· PO Box 217 · Elizabethtown, NY 12932· (518) 873-3441
Franklin County DSS
355 West Main Street, Suite 331 · Malone, NY 12953· (518) 483-6770 Website: https://franklincony.org/content/
Fulton County DSS
4 Daisy Lane · P.O. Box 549 · Johnstown, NY 12095 · (518) 736-5600
Genesee County DSS
5130 East Main St. Suite #3 · Batavia, NY 14020-3497· (585) 344-2580 Website: https://www.co.genesee.ny.us/dpt/socialservices/index.html
Greene County DSS
411 Main Street · P.O. Box 528 · Catskill, NY 12414-1716 · (518) 943-3200 Website: https://www.greenegovernment.com/department/socialserv/Hamilton County DSS
White Birch Lane · P.O. Box 725 · Indian Lake, NY 12842-0725 · (518) 648-6131
Herkimer County DSS
301 North Washington Street ·Site 2110 · Herkimer, NY 13350 · (315) 867-1222 Website: https://herkimercounty.org/content/Departments/View/10
Jefferson County DSS
Human Services Building · 250 Arsenal Street · Watertown, NY 13601 · (315) 782-9030
Lewis County DSS
Outer Stowe Street · P.O. Box 193 · Lowville, NY 13367 (315) 376-5400 Website: https://lewiscountyny.org/content/Departments/View/30?
Livingston County DSS
3 Murray Hill Drive · Mt. Morris, NY 14510-1699
(585) 243-7300 Website: https://www.co.livingston.state.ny.us/dss.htm
Madison County DSS
North Court St. · P.O. Box 637 · Wampsville, NY 13163 · (315) 366-2211 Website: https://www.madisoncounty.org
Monroe County DSS
111 Westfall Road – Room 660 · Rochester, NY 14620-4686 (585) 274-6000 Website: https://www.monroecounty.gov/hs-index.php
Montgomery County DSS
County Office Building · P.O. Box745 · Fonda, NY 12068 · (518) 853-4646
Nassau County DSS
60 Charles Lindbergh Blvd · Uniondale, NY 11553-3656
(516) 571-4444 Website: https://www.nassaucountyny.gov/agencies/dss/DSSHome.htm
NYC Administration for Children’s Services
150 William St. 18th Fl. · New York, NY 10038 (212) 341-0900 Website: https://www.nyc.gov/acs
Manhattan Field Office Application Unit
150 William Street – 3rd Floor New York, NY 10038
Brooklyn Field Office Application Unit
1274 Bedford Avenue- 2nd Floor Brooklyn, NY 11216
Queens Field Office Application Unit
165-15 Archer Avenue- 3rd Floor Jamaica, NY 11433
Staten Island Field Office Application Unit
350 St. Mark’s Place- 3rd Floor Staten Island, NY 10301
Bronx Field Office Application Unit 192 E 151st Street Bronx, NY 10451
Niagara County DSS
20 East Avenue P.O. Box 506 · Lockport, NY 14095-0506 · (716) 439-7600 Website: https://niagaracounty.com/departments.asp?City=Social+Services
Oneida County DSS
County Office Building · 800 Park Avenue · Utica, NY 13501-2981· (315) 798-5733 Website: https://www.ocgov.net/oneidacty/gov/dept/socialservices/dssindex.html
Onondaga County DSS
Onondaga Co. Civic Center · 421 Montgomery Street · Syracuse, NY 13202-2923 · (315) 435-2985 Website: https://www.ongov.net/DSS/
Ontario County DSS
3010 County Complex Drive · Canandaigua, NY 14424-1296 · (585) 396-4060 or Toll Free (877) 814-6907 Website: https://www.co.ontario.ny.us/social_services/
Orange County DSS
11 Quarry Road, Box Z · Goshen, NY 10924-0678 · (845) 291-4000
Website: https://www.co.orange.ny.us/orgMain.asp?orgid=55&storyTypeID=&sid=&
Orleans County DSS
14016 Route 31 West · Albion, NY 14411-9365 · (585) 589-7000
Website: https://orleansny.com/SocialServices/dss.htm
Oswego County DSS
100 Spring Street · Mexico, NY 13114 · (315) 963-5000 Website: https://www.co.oswego.ny.us/dss/
Otsego County DSS
County Office Building · 197 Main Street · Cooperstown, NY 13326-1196 · (607) 547-4355 Website: https://www.otsegocounty.com/depts/dss/
Putnam County DSS
110 Old Route Six Center, Building #2 · Carmel, NY 10512-2110 · (845) 225-7040 Website: https://www.putnamcountyny.com/socialservices/
Rensselaer County DSS
133 Bloomingrove Drive · Troy, NY 12180-8403 · (518) 283-2000 Website: https://www.rensco.com/departments_socialservices.asp
Rockland County DSS
Building L · Sanatorium Road · Pomona, NY 10970 · (845) 364-3100 Website: https://www.co.rockland.ny.us/Social/
Saint Regis Mohawk Tribe Human Services Division
412 State Route 37 · Akwesasne, NY 13655 · (518) 358-2209
Saratoga County DSS
152 West High Street · Ballston Spa, NY 12020 · (518) 884-4140
Schenectady County DSS
487 Nott Street · Schenectady, NY 12308 · (518) 388-4470
Website: https://www.schenectadycounty.com/index.php?page_id=378
Schoharie County DSS
County Office Building · P.O. Box 687 · Schoharie, NY 12157 · (518) 295-8334 Website: https://www.schohariecounty-ny.gov/CountyWebSite/index.jsp
Schuyler County DSS
County Office Building · 105 Ninth Street · Watkins Glen, NY 14891 · (607) 535-8303 Website: https://www.schuylercounty.us/dss.htm
Seneca County DSS
1 DiPronio Drive · P.O. Box 690 · Waterloo, NY 13165-0690 · (315) 539-1800 Website: https://www.co.seneca.ny.us/dpt-divhumserv-children-family.php
Steuben County DSS
3 East Pulteney Square · Bath, NY 14810 (607) 776-7611 Website: https://www.steubencony.org/dss.html
St. Lawrence County DSS
Harold B. Smith County Office Building · 6 Judson Street · Canton, NY 13617-1197 ·(315) 379-2111 Website: https://www.co.st-lawrence.ny.us/Social_Services/SLCSS.htm
Suffolk County DSS
P.O. Box 18100 · Hauppauge, NY 11788-8900· (631) 854-9700
Website: https://www.co.suffolk.ny.us/webtemp3.cfm?dept=17&ID=617
Sullivan County DSS
16 Community Lane · P.O. Box 231 · Liberty, NY 12754 · (845) 292-0100
Tioga County DSS
P.O. Box 240 · Owego, NY 13827 · (607) 687-8300
Website:https://www.tiogacountyny.com/departments/health/social_services/
Tompkins County DSS
320 West State Street · Ithaca, NY. 14850 · (607) 274-5252 Website:https://www.tompkins-co.org/departments/detail.aspx?DeptID=41
Ulster County DSS
1061 Development Court · Kingston, NY 12401-1959 · (845) 334-5000 W ebsite: https://www.co.ulster.ny.us/resources/socservices.html
Warren County DSS
Warren Co. Municipal Center · 1340 State Route 9 · Lake George, NY 12845-9803 · (518) 761-6300
Washington County DSS
Municipal Building · 383 Broadway · Fort Edward, NY 12828 · (518) 746-2300 Website: https://www.co.washington.ny.us/Departments/Dss/dss.htm
Wayne County DSS
77 Water Street · P.O. Box 10 · Lyons, NY 14489-0010 · (315) 946-4881 Website: https://www.co.wayne.ny.us/departments/dss/dss.htm
Westchester County DSS
County Office Building #2 · 112 East Post Road · White Plains, NY 10601-5113· (914) 995-5000 Website: https://www.westchestergov.com/health.htm
Wyoming County DSS
466 North Main Street · Warsaw, NY 14569-1080 · (716) 786-8900 Website: https://www.wyomingco.net/socialservices/main.htm
Yates County DSS
County Office Building · 417 Liberty Street, Suite 2122 · Penn Yan, NY 14527-1118 · (315) 536-5183 Website: https://www.yatescounty.org/upload/12/dss/frameset.html
More informational resources can be found at:
| American Professional Society on the Abuse of Children | This is a nonprofit national organization that focuses on helping professionals get what they need to help abused children and their families. They offer the latest in practices in all disciplines that are related to child abuse. |
| Child-Help USA | Treatment programs such as Child-help Group Homes and Child-help Advocacy centers have been designed to help children who are suffering from child abuse. There are also prevention programs, including Child-help Speak Up Be Safe for Educators. |
| Children’s Safety Network | This program offers resources and assistance to maternal and child health agencies that are looking to reduce violence towards children and reducing injuries that happen unintentionally. There are four Children’s Safety Network Resource Centers that are funded by the Maternal and Child Health Bureau of the US Department of Health and Human Services. |
| Darkness to Light | The mission of this program is to empower people to prevent child sexual abuse. It raises awareness of how common child sexual abuse is, and the consequences. Adults are educated so they know how to prevent this type of abuse, as well as recognize it and react appropriately. |
| Healthy Families America | This is the signature program from Prevent Child Abuse America. The national office, which is located in Chicago, IL, offer support, training, technical assistance, affiliation, and accreditation to more than 580 affiliates sites in 38 states, as well as the District of Columbia, American Samoa, Guam, Puerto Rico, Canada, and the Commonwealth of the Northern Mariana Islands. |
| International Society for Prevention of Child Abuse and Neglect | This organization has a mission to prevent cruelty to children in all parts of the world. Cruelty can include sexual abuse, physical abuse, neglect, child prostitution, street children, children of war, emotional abuse, child fatalities, and child labor through the increase of public awareness. |
| Kelso Lawyers | If you need to find more resources about child abuse, Kelso Lawyers can help. They offer resources for victims, such as symptoms of child sexual abuse, reporting abuse, abuse prevention, and causes of child sexual abuse. There are also resources for families, including child abuse statistics and child abuse counselling. |
| National Center for Missing and Exploited Children | This organization offers help to parents, children, schools, law enforcement, and the community to find missing children. It also works to raise public awareness about how to prevent child abduction, child molestation, and sexual exploitation. |
| National Center on Shaken Baby Syndrome | The mission of this organization is to help educate parents about the dangers of shaking babies, and to train parents and professionals on the subject. It also conducts research that will help to prevent the shaking of babies. The website is designed to help you find information, answers to questions about this issue, and ideas on how to prevent shaken baby syndrome. |
| Stop it Now | This program was founded by Fran Henry, who survived childhood sexual abuse herself. Her vision was to have sexual abuse of children seen as a preventable public health issue, to help parents focus on the prevention of abuse, and to create programs that are based on these same principles. |
| Administration for Children & Families | www.acf.dhhs.gov The Administration for Children and Families (ACF) is a federal agency funding state, territory, local, and tribal organizations to provide family assistance (welfare), child support, childcare, Head Start, child welfare, and other programs relating to children and families. |
| ACF – Children’s Bureau Express | www.cbexpress.acf.hhs.gov The Children’s Bureau Express is designed for professionals concerned with child abuse and neglect, child welfare, and adoption. The Children’s Bureau Express is supported by the Children’s Bureau, Administration for Children and Families, U.S. Department of Health and Human Services and published by the National Clearinghouse on Child Abuse and Neglect Information and the National Adoption Information Clearinghouse. |
| Annie E. Casey Foundation | www.aecf.org Since 1948, the Annie E. Casey Foundation (AECF) has worked to build better futures for disadvantaged children and their families in the United States. The primary mission of the Foundation is to foster public policies, human service reforms, and community supports that more effectively meet the needs of today’s vulnerable children and families. |
| Child Abuse Reporting | www.dorightbykids.org Monroe County Health and Human Services maintains a Website dedicated to learning about preventing and reporting child abuse |
| Child Welfare League of America | www.cwla.org The Child Welfare League of America is the nation’s oldest and largest membership-based child welfare organization. It is committed to engaging people everywhere in promoting the well-being of children, youth, and their families, and protecting every child from harm |
| Child Welfare Institute | www.gocwi.org This organization’s mission is to provide information, ideas, and guidance in the field of child welfare training and organizational development consultation. |
| National Children’s Alliance | www.nca-online.org The National Children’s Alliance is a group of 53 national organizations with an interest in the well-being of children and youth. |
| National Data Archive on Child Abuse & Neglect | www.ndacan.cornell.edu A resource since 1988, NDACAN promotes scholarly exchange among researchers in the child maltreatment field. NDACAN acquires microdata from leading researchers and national data collection efforts and makes these datasets available to the research community for secondary analysis. |
| New York State Office for Children and Family Services | www.ocfs.state.ny.us A variety of resource information related to child abuse and maltreatment/neglect specific to New York State. |
| U.S. Department of Health and Human Services | www.os.dhhs.gov |
- Ai, A. L., Lee, J., Solis, A., & Yap, C. (2016). Childhood abuse, religious involvement, and substance abuse among Latino-American men in the United States. International Journal of Behavioral Medicine, 23(6), 764-775. https://doi.org/10.1007/s12529-016-9561-z
- Alexander, R. A. (2011). Medical advances in child sexual abuse. Journal of Child Sexual Abuse, 20(5), 481-485. https://doi.org/10.1080/10538712.2011.607754
- Bozzay, M. L., Joy, L. N., & Verona, E. (2017). Family violence pathways and externalizing behavior in youth. Journal of Interpersonal Violence, 088626051772425. https://doi.org/10.1177/0886260517724251
- Bright, M. A., Knapp, C., Hinojosa, M. S., Alford, S., & Bonner, B. (2015). The comorbidity of physical, mental, and developmental conditions associated with childhood adversity: A population-based study. Maternal and Child Health Journal, 20(4), 843-853. https://doi.org/10.1007/s10995-015-1915-7
- Bright, M. A., & Thompson, L. A. (2017). Association of adverse childhood experiences with co-occurring health conditions in early childhood. Journal of Developmental & Behavioral Pediatrics, 1.
- NA; (2012). Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents-second edition. Pediatric Critical Care Medicine, 13, S1-S2. https://doi.org/10.1097/pcc.0b013e31823f435c
- Adelson, P. D., Wisniewski, S. R., Beca, J., Brown, S. D., Bell, M., Muizelaar, J. P., Okada, P., Beers, S. R., Balasubramani, G. K., & Hirtz, D. (2013). Comparison of hypothermia and normothermia after severe traumatic brain injury in children (Cool kids): A phase 3, randomized controlled trial. The Lancet Neurology, 12(6), 546-553. https://doi.org/10.1016/s1474-4422(13)70077-2
- Araki, T., Yokota, H., & Morita, A. (2017). Pediatric traumatic brain injury: Characteristic features, diagnosis, and management. Neurologia medico-chirurgica, 57(2), 82-93. https://doi.org/10.2176/nmc.ra.2016-0191
- Beaver, K. M. (2017). The interaction between genetic risk and childhood sexual abuse in the prediction of adolescent violent behavior. Biosocial Theories of Crime, 235-252. https://doi.org/10.4324/9781315096278-10
- Chen, C., Peng, J., Sribnick, E., Zhu, M., & Xiang, H. (2018). Trend of age-adjusted rates of pediatric traumatic brain injury in U.S. emergency departments from 2006 to 2013. International Journal of Environmental Research and Public Health, 15(6), 1171. https://doi.org/10.3390/ijerph15061171
- Guerrero, M. (2017). Accuracy of PECARN, CATCH, and chalice head injury decision rules in children: A prospective cohort study. The Journal of Emergency Medicine, 53(1), 155-156. https://doi.org/10.1016/j.jemermed.2017.05.015
- Mandated training related to child abuse. (n.d.). Office of the Professions | Office of the Professions. https://op.nysed.gov/professions/psychology/mandated-training-related-child-abuse
- Litz, C. N., Ciesla, D. J., Danielson, P. D., & Chandler, N. M. (2017). A closer look at non-accidental trauma: Caregiver assault compared to non-caregiver assault. Journal of Pediatric Surgery, 52(4), 625-627. https://doi.org/10.1016/j.jpedsurg.2016.08.026
- Mucha, A., DeWitt, J., & Greenspan, A. I. (2019). The CDC guideline on the diagnosis and management of mild traumatic brain injury among children: What physical therapists need to know. Physical Therapy, 99(10), 1278-1280. https://doi.org/10.1093/ptj/pzz085
- Rooney, E. E., Hill, R. M., Oosterhoff, B., & Kaplow, J. (2018). Violent victimization and perpetration as distinct risk factors for adolescent suicide attempts. https://doi.org/10.31234/osf.io/cgmqv
- Singhi, S., & Kumar, R. (2016). Raised intracranial pressure in children with an acute brain injury: Monitoring and management. Critical Care, 406-406. https://doi.org/10.5005/jp/books/12670_49
- Stockman, J. (2011). Identification of children at very low risk of clinically important brain injuries after head trauma: A prospective cohort study. Yearbook of Pediatrics, 2011, 392-395. https://doi.org/10.1016/s0084-3954(10)79686-x
- Taylor-Robinson, D. C., Straatmann, V. S., & Whitehead, M. (2018). Adverse childhood experiences or adverse childhood socioeconomic conditions? The Lancet Public Health, 3(6), e262-e263. https://doi.org/10.1016/s2468-2667(18)30094-x \
- Choudhary, S. (2025). Understanding the hidden signs of neglect and abuse in children with intellectual disabilities. International Journal of Research in Special Education, 5(1), 22-29. https://doi.org/10.22271/27103862.2025.v5.i1a.97
- DeBoer, M. I., Kothari, R., Kothari, C., Koestner, A. L., & Rohs, T. (2013). What are barriers to nurses screening for intimate partner violence? Journal of Trauma Nursing, 20(3), 155-160. https://doi.org/10.1097/jtn.0b013e3182a171b1
- Donohue, B., Alvarez, K. M., & Schubert, K. N. (2015). An evidence-supported approach to reporting child maltreatment. Mandatory Reporting Laws and the Identification of Severe Child Abuse and Neglect, 347-379.
- Kenny, M. C., & Abreu, R. L. (2015). Training mental health professionals in child sexual abuse: Curricular guidelines. Journal of Child Sexual Abuse, 24(5), 572-591. https://doi.org/10.1080/10538712.2015.1042185
- Kenny, M. C., Wurtele, S. K., & Alonso, L. (2012). Evaluation of a personal safety program with Latino preschoolers. Journal of Child Sexual Abuse, 21(4), 368-385. https://doi.org/10.1080/10538712.2012.675426
- Kuehnle, K., & Connell, M. (2010). Child sexual abuse suspicions: Treatment considerations during investigation. Journal of Child Sexual Abuse, 19(5), 554-571. https://doi.org/10.1080/10538712.2010.512554
- Litz, C. N., Ciesla, D. J., Danielson, P. D., & Chandler, N. M. (2017). A closer look at non-accidental trauma: Caregiver assault compared to non-caregiver assault. Journal of Pediatric Surgery, 52(4), 625-627.
To access 2025 NYSED Identification and Reporting of Child Abuse and Maltreatment/Neglect, purchase this course or a Full Access Pass.
If you already have an account, please sign in here.
To access 2025 NYSED Identification and Reporting of Child Abuse and Maltreatment/Neglect, purchase this course or a Full Access Pass.
If you already have an account, please sign in here.
FAQs
What is the NYSED Identification and Reporting of Child Abuse and Maltreatment course?
The NYSED Identification and Reporting of Child Abuse and Maltreatment course is required for healthcare professionals applying for licensure in New York. It teaches nurses how to recognize abuse, follow mandated reporting laws, and earn nursing CEUs for license renewal.
Who must complete the NYSED child abuse training?
Registered nurses, nurse practitioners, physicians, and other healthcare professionals must complete this training when applying for or renewing a New York license. Many providers offer the course through online nursing CEU courses for convenient learning.
Why is mandated reporter training important for nurses?
Mandated reporter training helps nurses recognize signs of abuse and neglect early. Completing continuing education for nurses online ensures healthcare professionals understand legal responsibilities and reporting procedures.
How many CEUs does this course provide?
Most courses provide around 2 nursing CEUs that count toward continuing education for nursing license renewal. These credits help nurses maintain professional compliance.
What signs of child abuse should nurses recognize?
Signs may include unexplained injuries, poor hygiene, behavioral changes, and emotional distress. Nurses learn to identify these warning signs through nursing continuing education online.
How do healthcare professionals report suspected abuse?
Healthcare providers report suspected abuse to Child Protective Services using hotline reporting and written documentation. This process is taught in continuing education courses for nurses
Are online CEU options available for this course?
Yes, many websites offer online CE and fast CEUs for mandated reporter training. Online courses allow nurses to complete required education at their own pace.
Does this course help with nurse license renewal?
Yes, the course provides CEUs for nursing license renewal. Completing it through online nursing CEU courses helps professionals meet state licensing requirements.